Tachycardia treated by an ATP burst
Patient
An 83-year-old man implanted with a Platinium DR in secondary prevention for sustained syncopal VT due to sequelae of inferior necrosis. The ejection fraction is maintained at 40%. This is a routine follow-up control, patient being asymptomatic. However, the
patient has already received a shock due to sustained ventricular tachycardia.
You interrogate the device

Trace
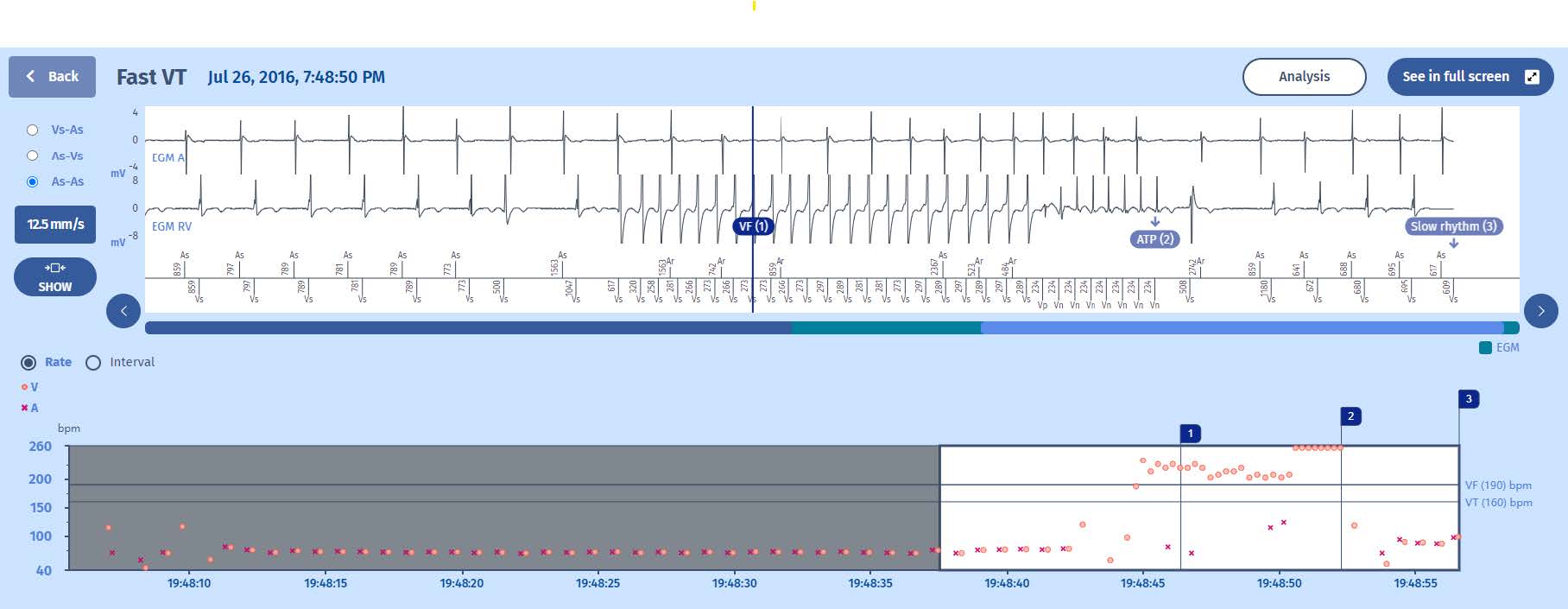
Interval plot
Sinus rhythm with A-V association
1 Beginning of a ventricular rhythm in the VF zone
2 Triggering of an ATP
3 Return to the slow zone

EGM
1 The rhythm is sinus, conducted (As-Vs);
2 Sudden onset of ventricular tachycardia detected in the VF zone. The first 6 cycles immediately indicate a VF. The next 15 are the persistence cycles as programmed.
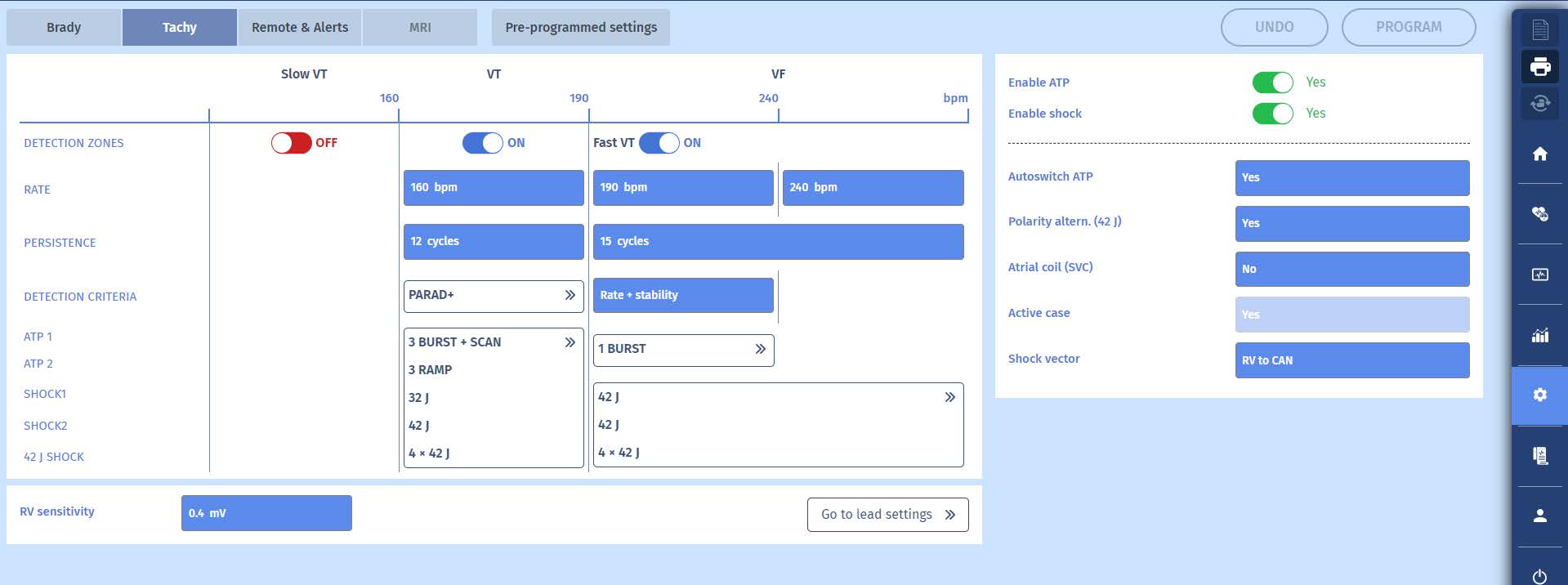
3 The tachycardia is stable and situated between the programmed values of 190 and 240 per minute. An ATP burst is delivered with 8 cycles and a coupling interval equal to 80% of the tachycardia coupling (292 ms for the VT, hence 234 ms for the burst).
4 The rhythm is slow over 6 cycles confirming the end of the episode.
Comments
Comments
1 This case demonstrates the benefit of antitachycardia pacing in the VF zone. This very fast tachycardia is not ventricular fibrillation but rather monomorphic ventricular tachycardia; treatable by rapid pacing.
2 As always, the problem remains whether the ATP will be effective and thus avoids the delivery of a shock, or whether it will delay this shock after the ineffectiveness of the ATP. In this example, the ATP is effective.
3 The burst did not generate capture during the first cycle. During the first three cycles, there is a fusion between the spontaneous depolarization of the tachycardia circuit and the depolarization generated by the pacing from the implantation site of the right
ventricular defibrillation lead. As a result, only the last cycles of the burst have a chance to penetrate the tachycardia circuit and influence the heart rate. It may therefore be necessary to program a larger number of cycles during the burst which may render it
more effective. The risk is that, on the contrary, the increase in the number of cycles transforms the tachycardia into fibrillation that will need to be shocked. The result is thus case by case and cannot be predicted before trying it. In the present example,
there is no reason to change the therapy.
4 The tachycardia episode is very short, thus raising the question of whether it would have terminated spontaneously. In order to allow this opportunity, it would be necessary, in this instance, to increase the number of persistence cycles. On the other hand, given that we are in the VF zone, extending the duration of the analysis may also delay the start of effective treatment. However, it has been shown that lengthening the analysis time prior to therapy does not change the prognosis.
Take home message
Programming an antitachycardia burst prior to the charging of the capacitors on a fast monomorphic tachycardia provides an opportunity to avoid delivering a defibrillation shock
Programming a large number of cycles before initiating therapy may allow spontaneous termination of the tachycardia without defibrillator intervention.
In the VF zone, in the fast VT section, if the tachycardia is stable, an ATP sequence is called upon before the shocks.

