75-year-old man implanted with an Energen single-chamber defibrillator; episode recorded in device memory
EGM layout
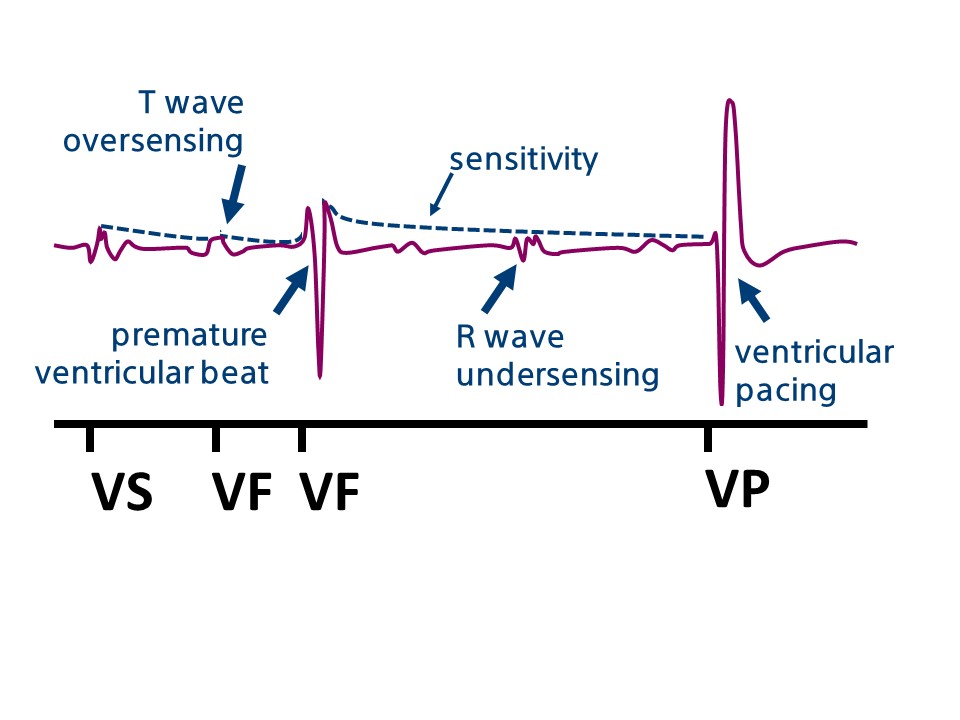
sinus rhythm with intermittent T wave oversensing
prolonged oversensing and 8/10 criterion verified (V-Epsd)
end of duration (1 second) and start of capacitor charging
ventricular extrasystole and under- sensing of the following QRS complex
undersensing and interruption of charging
criterion 8/10 checked again; at the end of the duration, ATP Quick Convert
charge diversion in the absence of oversensing
Take home message
although T wave oversensing remains a significant problem in the management of patients implanted with a defibrillator, this type of oversensing, which is fairly frequent with some brands, is very rare with Boston ScientificTM devices; in fact, the majority of clinicians managing this type of defibrillator have never observed it.
T wave oversensing is associated with a typical alternation between 2 morphologically different signals, a high-frequency signal (R wave) and a low-frequency signal (T wave); for each cardiac cycle, the device counts the R wave and then the T wave as a second additional signal, resulting in a doubling of the heart rate; the alternating cycle length (RT intervals and TR intervals) is generally marked for slow heart rates (short RT intervals and long TR intervals) but is often less marked during exercise (RT and TR intervals approximately equivalent) or for patients with a long QT
T wave oversensing is more likely if the preceding R wave is of small amplitude (as in this patient); in fact, when the R wave is of small amplitude, the device rapidly reaches high levels of sensitivity, favoring T wave oversensing, particularly during exercise (which may result in a reduced R wave amplitude and a slight increase in the T wave amplitude); there are few reprogramming options in this context (no possibility of modifying filters, or reprogramming the adaptation level or delay, or margin to adjust the ventricular sensitivity); these situations are therefore difficult and any programming change compromises another aspect of programming; it may therefore be necessary to reposition the lead.
This figure shows T wave oversensing following a small amplitude R wave and then the occurrence of an extrasystole with under-sensing of the R wave which follows.