Male with ischaemic cardiomyopathy, implanted with a Momentum triple-chamber defibrillator; aortic valve replacement surgery; trace recorded during the procedure
Summary
detection of an episode in the VF zone
no therapy delivered (device not programmed for monitoring + treatment)
EGM layout
no atrial or ventricular activity visible on the 3 channels; baseline interference explains the sensing of intermittent signals on the atrial and ventricular channels
simultaneous sensing on the 3 channels (atrial, ventricular, shock) of fast, chaotic signals of variable amplitude and morphology (classified as AF, VF) when electrocautery is used by the surgeon.
Patient 2
male implanted with an Autogen triple-chamber defibrillator; cardiac surgery (coronary bypass); trace recorded during the procedure
Summary
detection of an episode in the VF zone
electric shock of 41 Joules
EGM layout
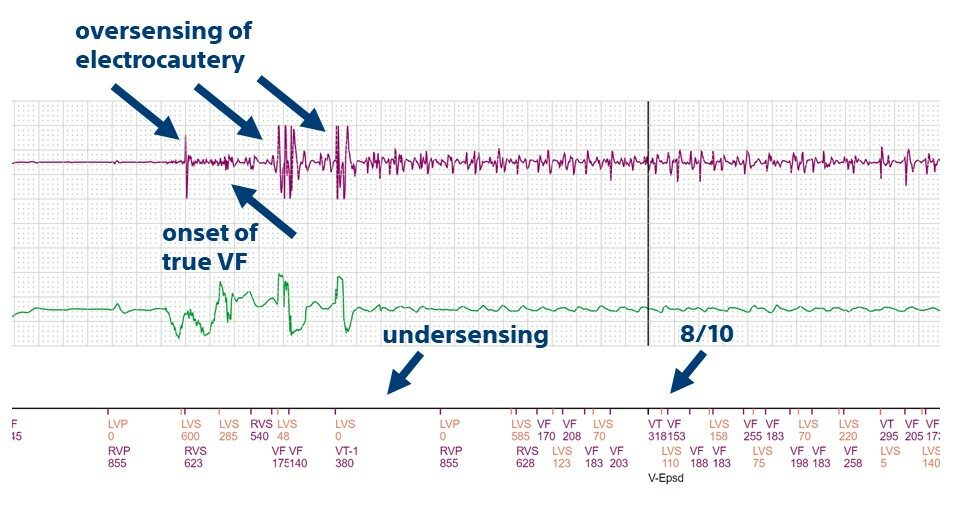
simultaneous detection of fast, chaotic signals of variable amplitudes and morphology on the ventricular and shock channels (electrocautery)
end of oversensing
onset of a very rapid, low voltage ventricular arrhythmia; imperfect ventricular sensing
detection of a VF episode and capacitor charging
electric shock of 41 Joules
termination arrhythmia
Take home message
these 2 patients underwent cardiac surgery with extra-corporeal circulation; for the first patient, the Tachy Mode was programmed to monitor only during the procedure, for the second to monitoring + treatment; it is usual to program the Tachy Mode to off, with any bradycardia or tachycardia occurring during the procedure being managed by temporary pacing or external cardioversion respectively.
the first tracing shows a characteristic appearance of cardioplegia (asystole despite the pacing delivered by the defibrillator); this technique, which aims to stop the activity of the heart during the operation, is carried out by injecting a liquid very rich in potassium directly into the coronary arteries; this makes it possible to carry out the surgical procedure on immobile organs; the first tracing shows, overlying this flat background trace, the oversensing of characteristic signals related to the use of electrocautery by the surgeon
the second trace shows the detection and termination of a true VF episode by a shock delivered by the device; this arrhythmia occurs during reperfusion at the end of the operation, which is relatively frequent and is usually managed by the anesthetic team with external defibrillation, the implantable device having been deprogrammed before the operation.
This figure shows the characteristic appearance of cardioplegia followed by oversensing of electrocautery and then the onset of true VF.