

Programming

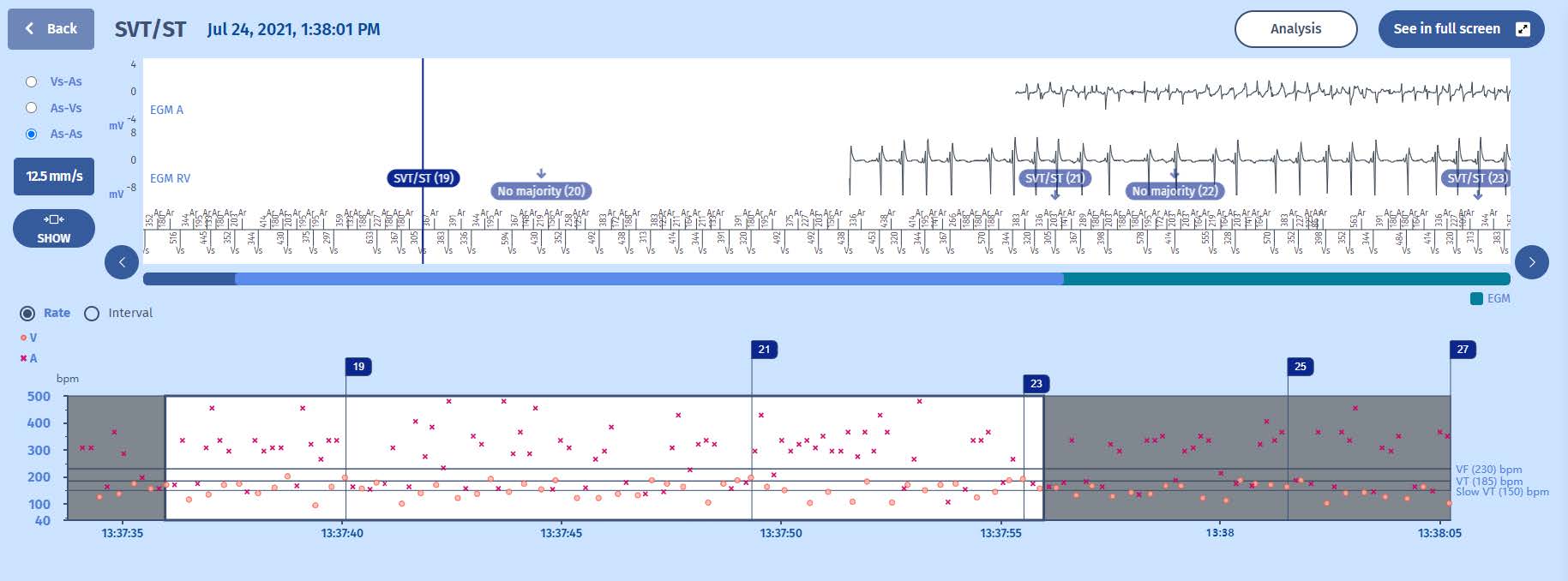
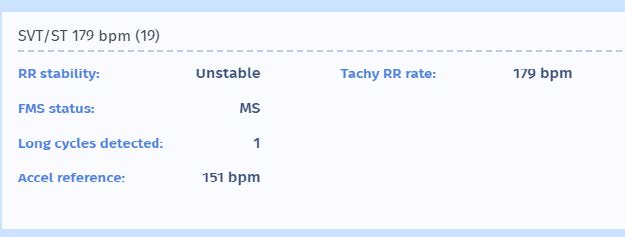
For marker 19, we can appreciate that the diagnosis of “SVT/ST” was made as the ventricular events were considered “unstable”. Again working with the “majority” method, 6 out of 8 ventricular events surpassed the 65 ms threshold, as programmed in the discrimination screen:
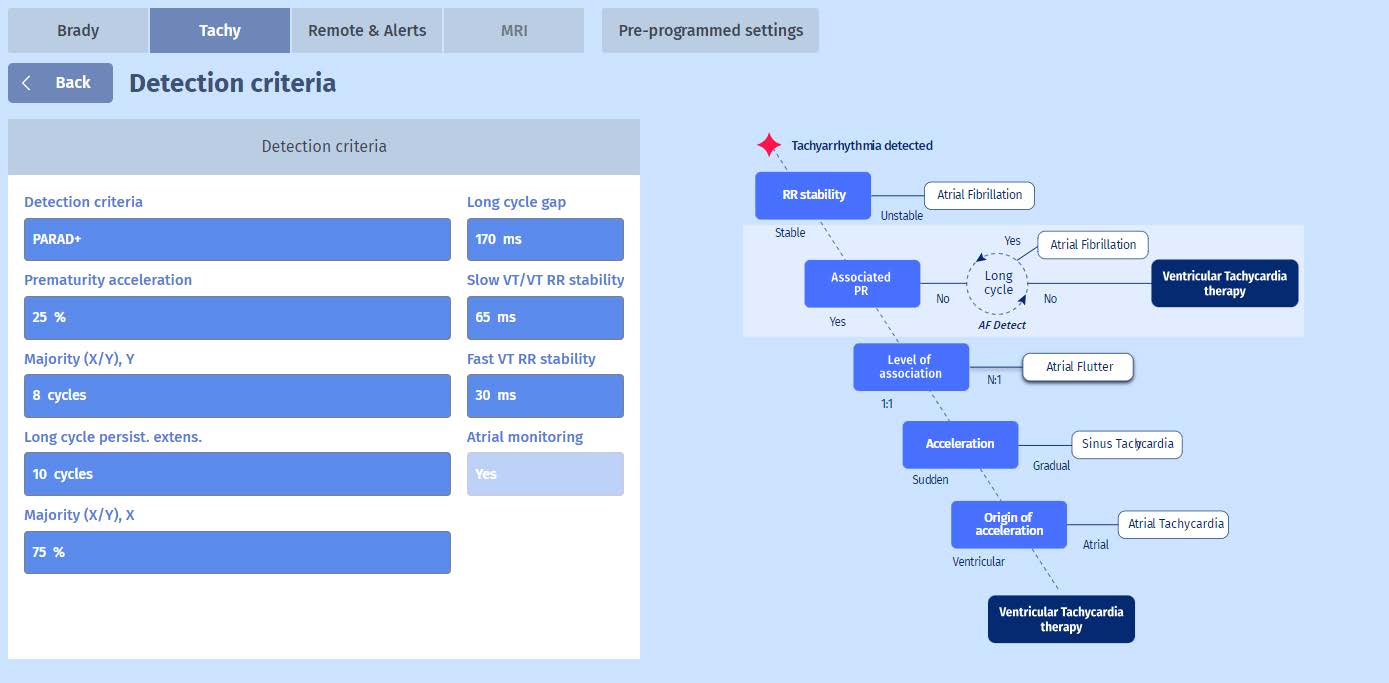
We can appreciate the importance of “Stability” in the PARAD+ discrimination algorithm tree on the right of the figure, as it is the first step. When the VT criteria are met but RR is instable, it is considered as AF, the episode is saved as “SVT/VT” and therapy is withheld. This also holds true for slow VT zones without therapies, such as in this case. As the episode continues, we can imagine that in some instances, the rapid ventricular events in fact become stable enough to not cross the 65 ms threshold. This is indeed true in this episode for example for marker 21.
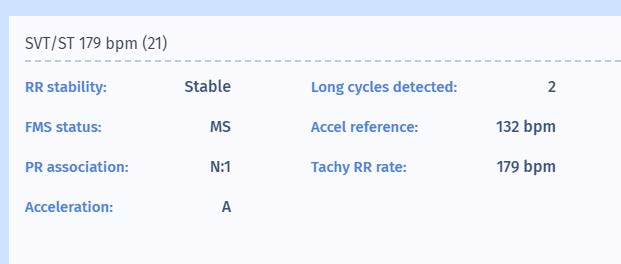
We can learn from the figure that marker 21 is considered as “Stable”. Fortunately, the PARAD+ has more criterion which protects against inappropriate diagnosis of VT in case of AF with rapid ventricular response. It is actually looking for atrioventricular association and in this case, finds that the relation is N:1, declaring it as supraventricular. It also correctly identified the origin of the tachycardia as atrial, which can also help in correctly discriminating the episode as
supraventricular.