male with ischemic cardiomyopathy implanted with a Resonate single-chamber defibrillator
Summary
episode classified in the VF zone
ATP in the VF zone
diverted shock
EGM layout
spontaneous polymorphic ventricular arrhythmia
V-Epsd marker (criterion 8/10 fulfilled) for VT-1 zone (1 VT-1 cycle, 5 VT cycles, 2 VF cycles)
8/10 criterion for the VT zone; the initial detection time for the VT zone begins on this beat
8/10 criterion for the VF zone; initial detection time for the VF zone begins on this beat
end of duration for the VF zone; burst in the VF zone (ATP Quick-Convert)
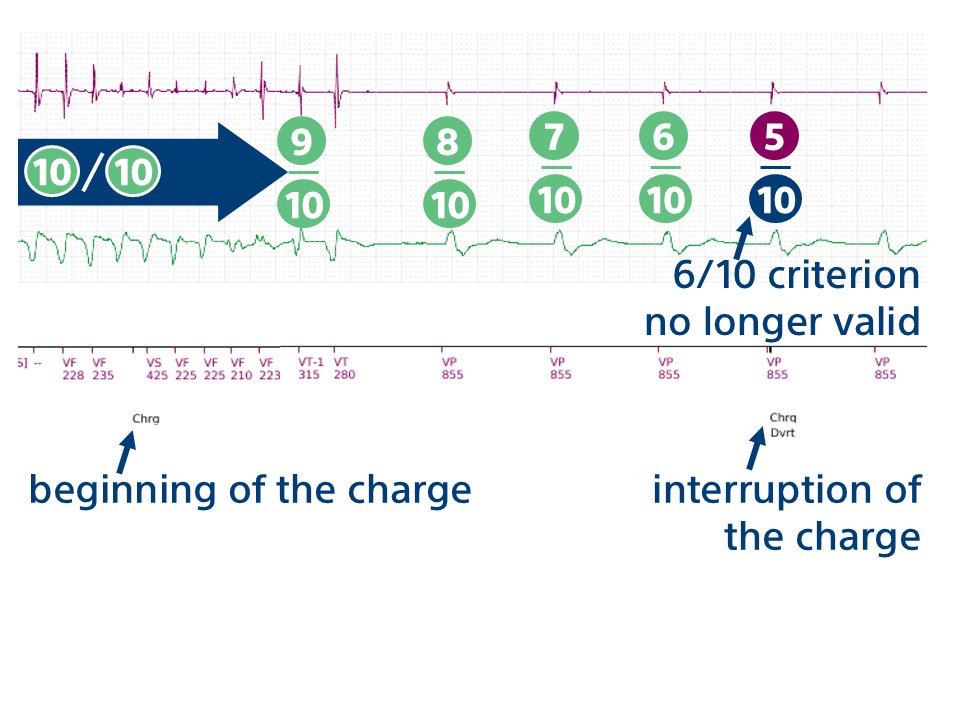
ineffective burst and start of capacitor charging
spontaneous termination
criterion 6/10 no longer fulfilled; charge diverted
Patient 2
male with ischemic cardiomyopathy; implanted with Autogen dual-chamber defibrillator
Summary
episode classified in the VF zone
ATP in the VF zone
diverted charge
EGM layout
sinus rhythm and ventricular pacing
ventricular extrasystole occurring in the ventricular noise window after atrial pacing (VS marker in square brackets); no pacing inhibition and ventricular pacing (VP) at the end of the programmed AV delay.
spontaneous polymorphic ventricular arrhythmia
V-Epsd marker (criterion 8/10 fulfilled); criterion fulfilled for VT-1 zone (1 cycle in VT-1 zone + 1 cycle in VT zone + 6 cycles in VF zone); initial detection time for VT-1 zone begins on this beat
8/10 criterion for VT zone; initial detection time for the VT zone begins on this beat
8/10 criterion for VF zone; initial detection time for the VF zone begins on this beat
end of duration for VF zone
burst in VF zone (ATP Quick-Convert)
ineffective burst and start of capacitor charging
spontaneous termination
end of charge and start of 500 ms diversion window
the first ventricular cycle following the 135 ms end-of-charge blanking is not counted (–)
2 slow cycles out of 3; diverted charge
Take home message
the main aim of programming is to reduce, as far as possible, the number of inappropriate or avoidable therapies; programming an initial duration of 5 seconds in the VF zone and a first shock of maximum output as first-line treatment (i.e. with a charge duration of more than 8 seconds) extends the delay between the onset of arrhythmia and shock delivery, allowing spontaneous termination; these 2 tracings show 2 episodes of ventricular arrhythmia with spontaneous termination and interruption of charging or charge diversion after the diversion window
shock therapy can be programmed to be reconfirmed or not reconfirmed; the aim of reconfirmation is to prevent delivery of an unnecessary shock when the arrhythmia has spontaneously terminated; the device looks for spontaneous termination during and immediately after capacitor charging
if the Shock not reconfirmed function is set to On, the shock is systematically delivered synchronized to the first sensed R wave following a 500 ms delay at the end of capacitor charging (whether the arrhythmia is sustained or not); therefore, if capacitor charging begins, the shock is automatically delivered
if the Shock not reconfirmed function is set to Off, charging can be interrupted if the device diagnoses spontaneous termination; if 5 slow beats (sensed or paced) are counted within a detection window of 10 beats (6/10 fast criterion not fulfilled), the device interrupts charging (first trace); if the charge has been completed, post-charge reconfirmation is performed at the end of the charge; after the post-charge refractory period and the first uncounted sensed event, if 2 of the 3 post-charge intervals have a rate below the lowest rate threshold, the shock is not delivered.
This figure shows the charge interruption following spontaneous reduction and the detection of 5 consecutive slow cycles.