Single-chamber discrimination, Rhythm ID and a ventricular tachycardia episode - Resonate ICD
Patient
- 43-year-old male; ischemic cardiomyopathy; implanted with Resonate single-chamber defibrillator
Summary
- discrimination based on Rhythm ID (threshold programmed at 94%)
- episode diagnosed as VT at a rate of 217 beats/minute
- no correlation between tachycardia ventricular electrogram morphology and reference morphology (Rhythm ID correlated: False)
- episode treated with a burst of ATP
EGM layout
- abrupt onset of a relatively stable tachycardia (rate above 200 beats/minute) with a different morphology on the shock channel compared to the ventricular electrogram in sinus rhythm
- start of morphology analysis; no correlation (U = uncorrelated) with reference morphology (0%)
- V-Epsd marker after 8 cycles classified as VT; start of initial duration for VT zone (12 seconds)
- end of duration; V-detect marker; discrimination (RID-) is in favor of VT; the vector is correlated with the reference vector for fewer than 3 of 10 beats in a rolling window (none of the last 10 ventricular complexes before the end of the duration are correlated).
- ATP burst
- effective burst and arrhythmia termination
Take home message
- the initial detection of an arrhythmia episode is based on rate and duration criteria; the concept of heart rate is essential, but too simplistic to differentiate between ventricular and supra-ventricular arrhythmias; implementation of a heart rate criterion on its own carries a sensitivity of 100%, but limited specificity of no more than 60%; improving specificity therefore relies on discrimination, which is the ability of a defibrillator to identify a supra-ventricular or ventricular origin for an episode of tachycardia, based on the characteristics of the detected arrhythmia.
- discrimination algorithms should only be programmed in patients likely to present with conducted supraventricular tachycardia, and should be deactivated in patients with complete and permanent atrioventricular block where any spontaneous rapid rhythm can only be of ventricular origin
- if all discrimination criteria are disabled, therapy is delivered regardless of the origin of the tachycardia
- for Boston ScientificTM devices, the discrimination algorithms are only functional in VT zones (VT and/or VT-1); in the VF zone, a safety first approach prevails and the detection by the defibrillator of a high ventricular rate entering the «VF detected» zone triggers the programmed therapies, without the episode being «filtered» by discrimination algorithms
- the detection of an arrhythmia episode, whether supraventricular or ventricular, triggers the storage of an endocardial electrogram that is accessible during defibrillator interrogation; this enables critical analysis of the defibrillator’s diagnostic conclusions and possible reprogramming in the event of tachycardia misclassification
- 2 different «packages» are available on Boston ScientificTM defibrillators to enable discrimination of arrhythmia origin: the Rhythm ID algorithm and the Onset/Stability algorithm; the Rhythm ID discrimination option is available in isolation (only discriminant used) on a single-chamber defibrillator and is based on a comparison between ventricular vectors in tachycardia and a reference vector recorded outside a tachycardia episode.
- the performance of a discrimination algorithm is assessed based on its sensitivity (ability to correctly diagnose a VT; this should be as close as possible to 100%; a sensitivity of 95% means that 5% of VTs will be incorrectly diagnosed as SVT) and specificity (ability to inhibit therapies for an episode of SVT; this should be as high as possible without altering sensitivity).
- in this example of appropriate therapy for VT, the difference in morphology between sinus rhythm and tachycardia was obvious; the nominal threshold value of 94% was programmed and all tachycardia vectors were deemed uncorrelated, explaining the diagnosis of VT and the decision to treat
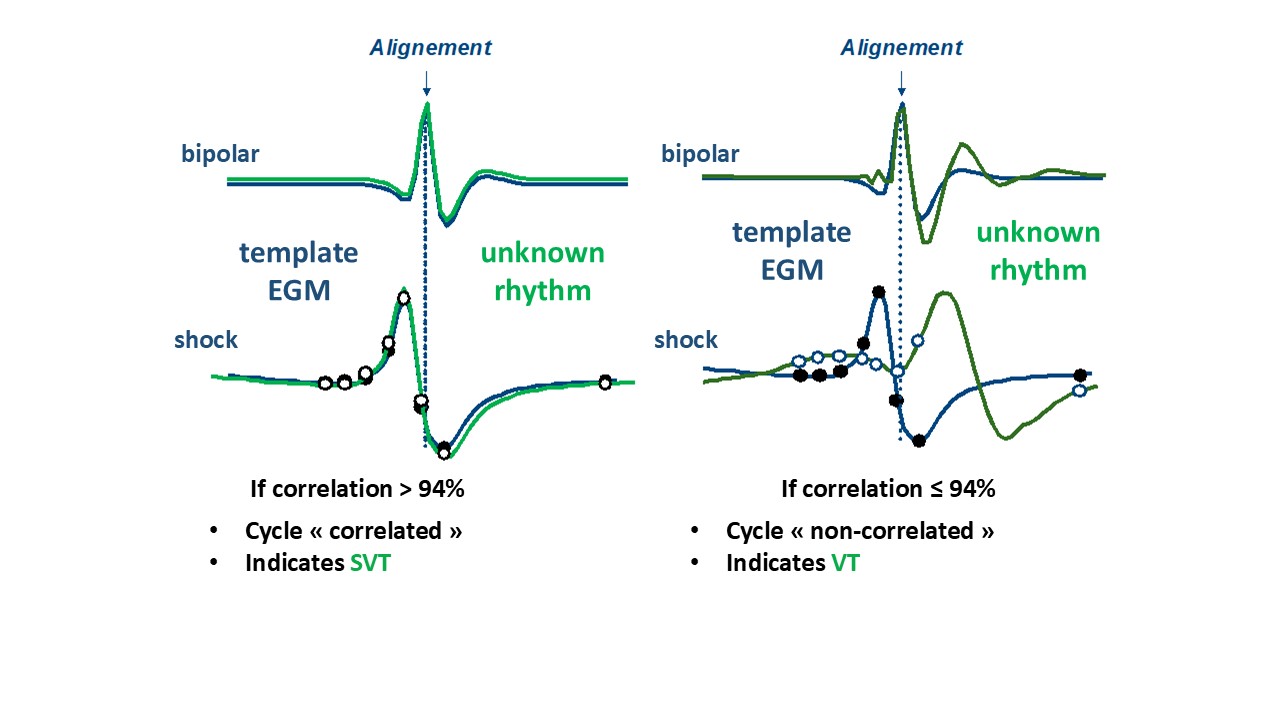
Operating principle of Rhythm-ID discriminantion: comparison between ventricular vectors in tachycardia and a reference vector; the bipolar sensing EGM enables alignment (localization of QRS peaks), and the comparison is made on the shock channel (decomposition of the QRS complex into 8 equidistant points).

