73-year-old woman implanted with a Resonate CRT defibrillator
Summary
episode classified in the VT zone
4 bursts + 4 ramps + 1 shock of 11 Joules
EGM layout
spontaneous atrial rhythm and biventricular pacing
monomorphic, regular ventricular tachycardia (atrioventricular dissociation) diagnosed in the VT zone
V-Epsd after 8 out of 10 cycles in the VT zone and start of initial VT zone duration (12 seconds)
diagnosis of sustained VT (V-Detect) at end of duration (V>A)
burst of 10 complexes at fixed rate; biventricular pacing
ineffective burst and ongoing arrhythmia
criterion 8/10 verified and start of post-detection time (1 second)
end of duration, second burst
ineffective burst
criterion 8/10 verified and start of post-detection time (1 second)
third burst
fourth burst
first ramp
second ramp
third ramp
effective ramp
restart of an identical VT before the V-EpsdEnd marker
fourth ramp (the device considers this to be the same episode)
next therapy is a shock; capacitor charging begins
end of charge
shock delivered after the end of the diversion window on the second rapid ventricular cycle (2/3 rapid cycle criterion verified)
effective shock
Take home message
during this episode, the first sequences of anti-tachycardia pacing fail to terminate the arrhythmia; as in the previous trace, anti-tachycardia pacing is then effective, but the tachycardia recurs before the end-of-episode marker, and successive therapies follow until a shock is delivered ; the programming of ramps following bursts is not systematic for this rate range since it is more aggressive with an increased risk of acceleration into a rapid polymorphic tachycardia
To optimize the effectiveness of anti-tachycardia pacing, various parameters can be programmed:
type of sequence : in a burst, the interval duration is constant during a sequence (no change in frequency from one stimulus to the next); in a ramp, the interval is reduced from one stimulus to the next by the value of the programmable decrement;
the number of bursts/ramps programmed varies according to the rate of the tachycardia; it is possible to program 2 burst or ramp sequences per VT or VT-1 zone; in a slow VT zone (< 150 beats/minute), it is possible to program a large number of bursts and/or ramps, to delay as long as possible shock delivery to a tachycardia that does not generally threaten short-term survival; for tachycardias between 150 and 200 beats/minute, it is usual to program 2 to 6 bursts/ramps, even if the success rate beyond 3 or 4 bursts is very limited;
the number of pulses per sequence: on average, 5 to 15 consecutive pacing impulses are programmed in each burst; if the number is too low, the stimulation sequence may not penetrate the tachycardia circuit and the burst is ineffective; on the other hand, if the number is too high, there is a risk of terminating and then re-inducing the tachycardia; an additional stimulus can be added systematically from one sequence to the next; according to the guidelines, a minimum number of 8 stimuli per sequence should be programmed;
the value of coupling and pacing intervals: the shorter the coupling, the more aggressive the therapy and the greater the risk of accelerating the tachycardia; according to the guidelines, for a burst, a coupling of 88% in relation to the rate of the tachycardia should be programmed; for Boston Scientific defibrillators, the coupling interval (interval between the last tachycardia cycle and the first pacing cycle) and the pacing interval (interval between different paced impulses) are independently programmable; the percentage is calculated in relation to the average of the 4 intervals preceding therapy;
minimum coupling limits the aggressiveness of a stimulation sequence; there is a programmable rate limit above which, regardless of programming, the device will not deliver stimulation; when, during a ramp for example, the minimum coupling interval is reached, subsequent cycles are paced with this minimum coupling interval without further decrementing;
stimulation amplitude and pulse duration can be programmed to favor effective capture during tachycardia (5 Volts/1 ms);
maximum duration for ATP : this defines the time after which ATP sequences will be interrupted to deliver a shock; the idea is not to delay the onset of the first shock by too many ATP sequences.
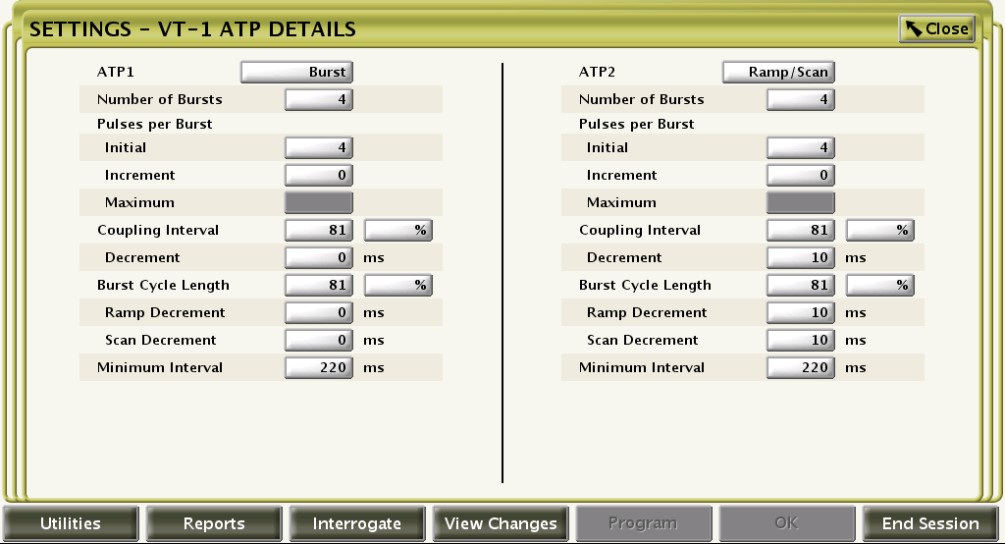
This figure shows the various programming options for optimizing the effectiveness of the anti-tachycardia pacing sequence(s).