

A 60-year old patient implanted with a CRT-D because of dilated cardiomyopathy with left bundle branch block, visits our clinic for a device check. The patient has sensed short bursts of palpitaitons lately.
You interrogate the ICD

This is one of the episodes responsible for palpitations, set to 12,5 mm/sec:
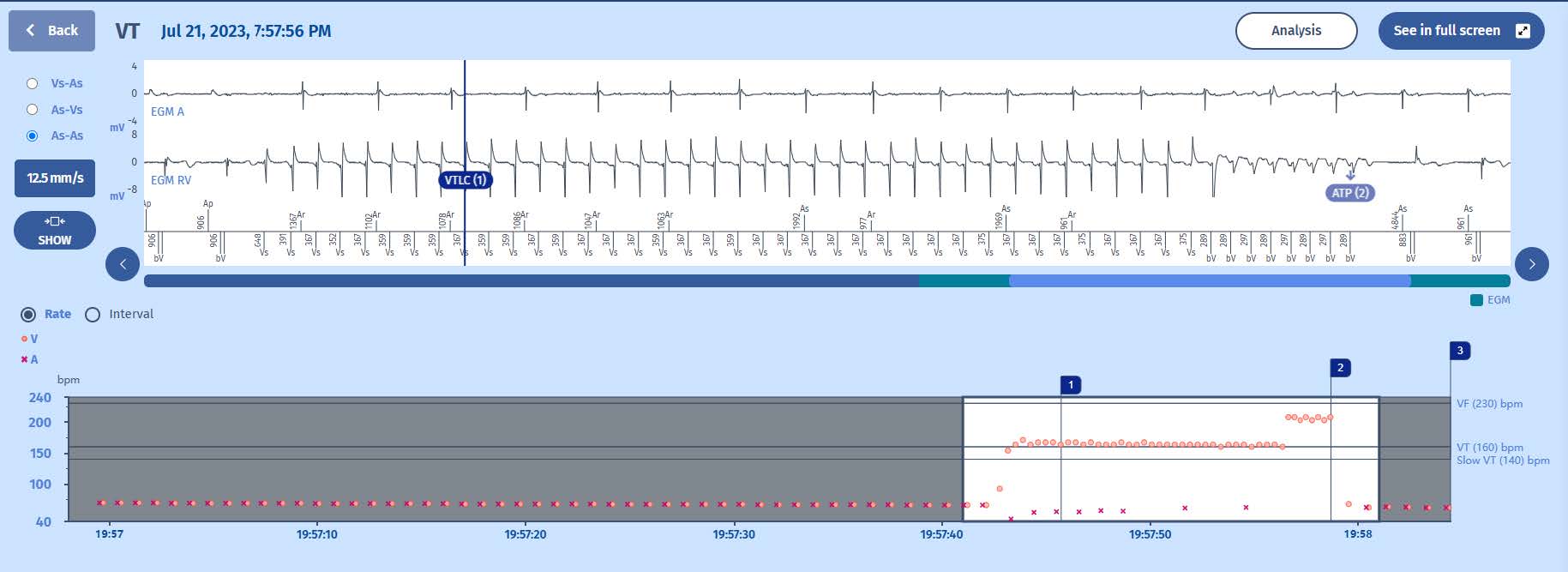
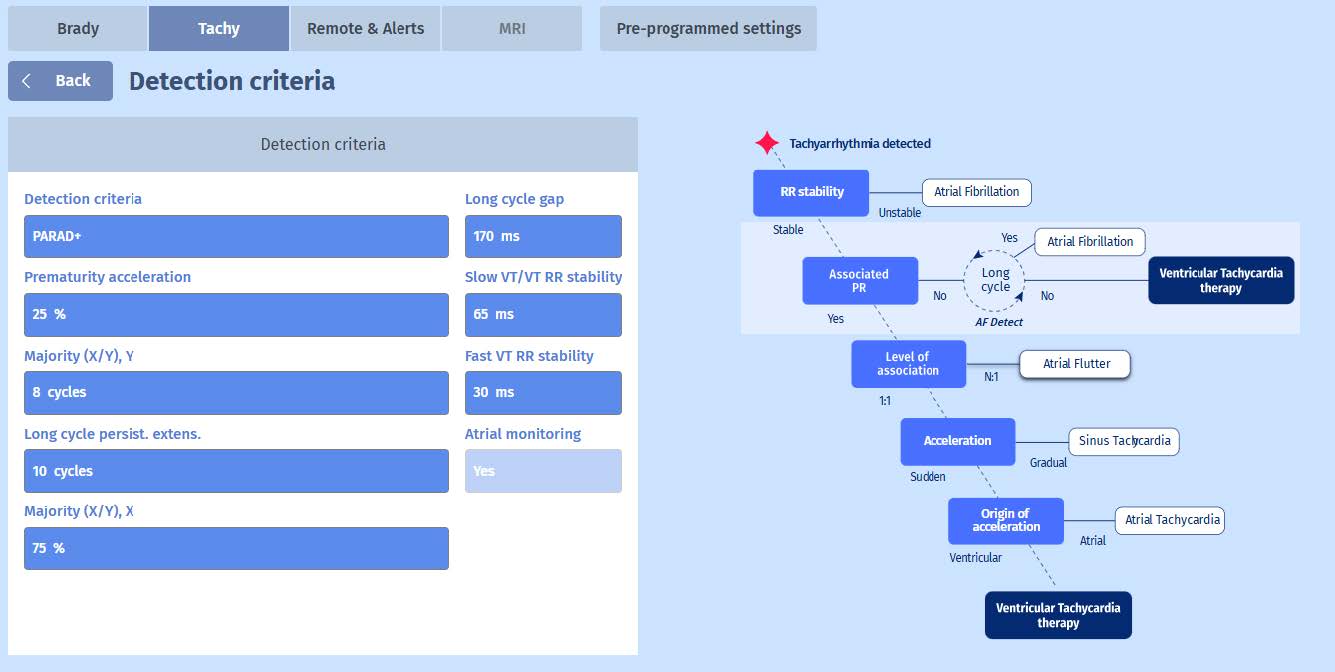
We see that when a Tachyarrhythmia is detected, the PARAD+ will first check whether the rhythm is stable. Since AF is the most important supraventricular tachycardia to cause inappropriate therapies, this is the first step in the PARAD+ algorithm. The second step is to verify whether the atria and ventricles are associated. In the case of most VTs, there is no association and therefore this is a good criterion to distinguish between VT and SVT. To verify which route the PARAD+ algorithm took in this example, we can click on Analysis on the programmer screen and it will display the following information.

We can see that the ventricular rhythm was indeed considered as stable (PARAD+ step 1) and that there is no PR association (step 2). This is how the diagnosis of VT is made.
Why the “LC” in VTLC?
Stability and lack of PR association is a powerful combination for discrimination but the pitfal remains AF with soo rapid ventricular conduction that it may become quite “stable”. This is when the engineers decided to upgrade PARAD to PARAD+ with the search for long cycles. A cycle is considered long when it is 170 ms (programmable) longer than the mean coupling interval of the VT. This serarch is associated to an increase of the initial persistence counter by 10 cycles (programmable, see PARAD+ figure). If PARAD+ is programmed and the diagnosis of VT has been made following these steps, the VTLC marker appears to show that it has used the long cycle criterion. We can consider it as another safety measure against inappropriate therapies due to AF
with fast ventricular conduction.