

Overview sceen

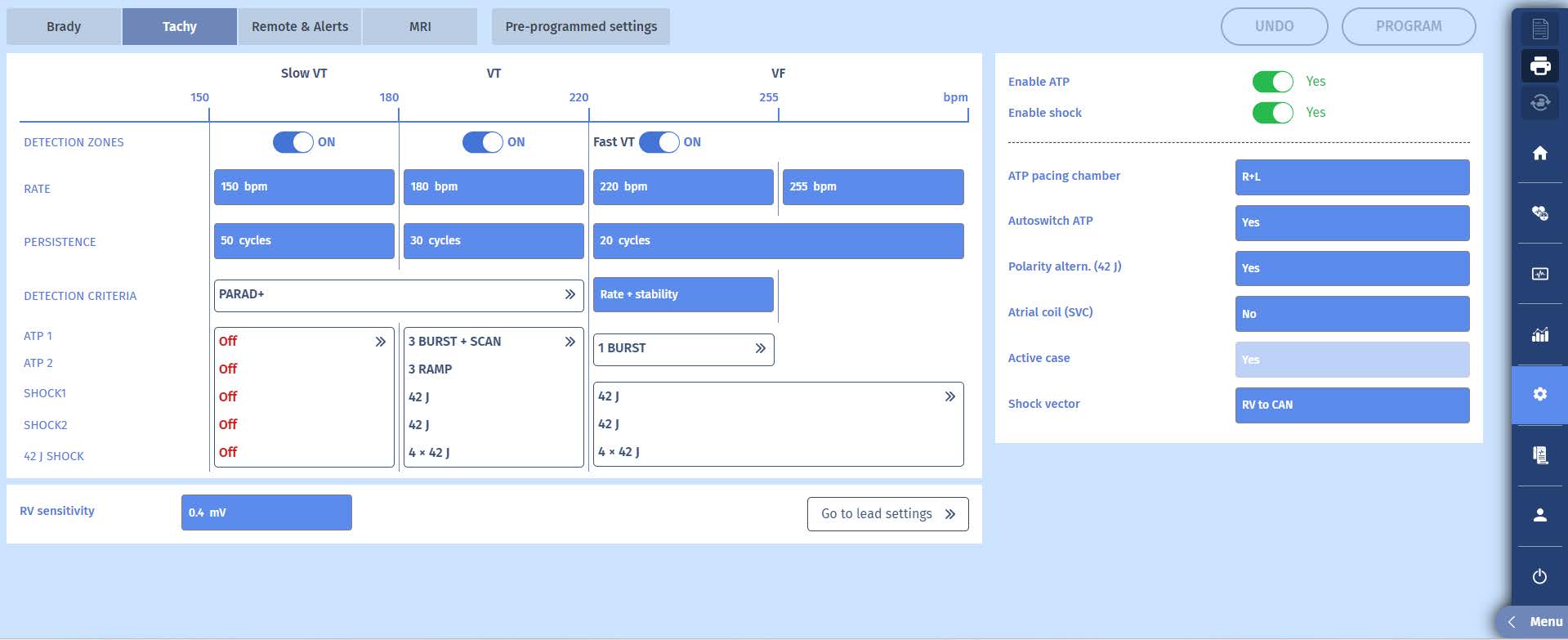
The programmer screen shows well functioning leads and a single episode which received treatment.
This is the episode:
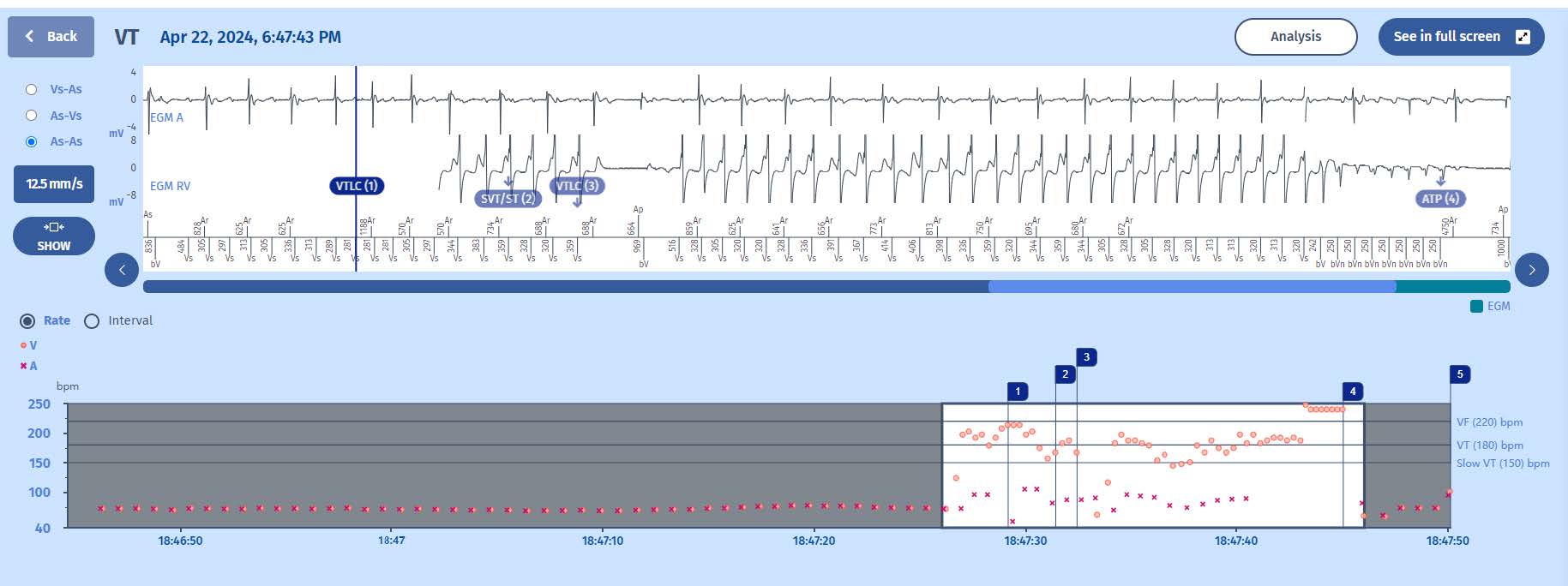
Tachogram
After an slow and regular rhythm suggesting atrial sensing and biventricular pacing, there is a sudden acceleration of ventricular cycles. As there are more ventricular events than atrial events, the episode is highly suspicious of ventricular tachycardia, in the VT zone. Marker 1-3 are related to counters and marker 4 is an ATP, which is succesful.
EGM
1 The rate of the initial rhythm around 70 beats per minute
2 then the diagnosis of VT (Marker 1: VTLC) is made after 6 out of 8 cycles in the VT zone.
3 the rhythm becomes irregular, the ICD suspects atrial fibrillation and so displays the second marker: SVT/ST
4 after a few more cycles, the rhythm again stabilises and the third marker shows: VT
5 when the persistence counter is completed (more details about this later), an ATP is delivered (burst with 8 pulses) which terminates the VT
6 after 6/8 slow events, marker 5 marks the end of the episode
The persistence counter is essential for two reasons.
1 It prevents unnecessary therapy by allowing nonsustained ventricular arrhythmias to self terminate. Multiple studies have shown that treatment of ventricular tachycardias by shocks is deleterious for the patient. Shock may be delivered because ATPs are
not succesful but also because ATP may even accelerate the arrhythmia into the VF zone. All efforts need to be made to avoid ICDs treating VT and programming a long persistence is probably the most efficient method. In the VT zone the persistence
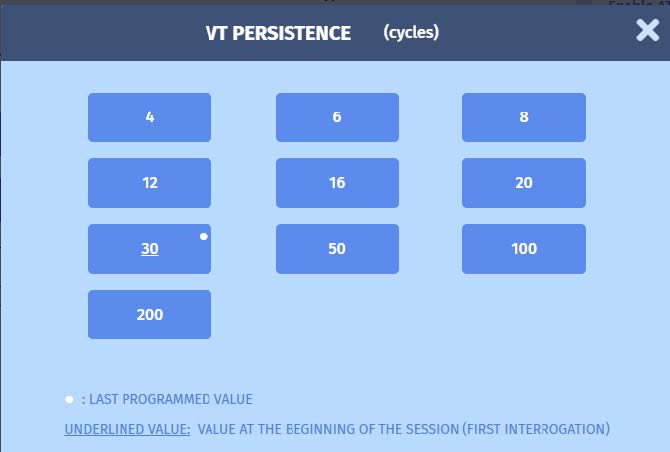
should be programmed at 20 or 30 but it can even programmed to 200.
2 It prevents inappropriate therapy by allowing for supraventricular arrhythmia or noise to self terminate before the wrong diagnosis (VT or VF) is made. Noise is often expressed as short bursts of ventricular oversensing and programming a persistence of 20 cycles or more is very efficient in preventing the filling of the persistence counter during bursts of noise. Supraventricular arrhythmias can be errounously diagnosed as VT for many reasons and a longer persistence counter gives the ICD more chance to rediagnose the arrhythmia as supraventricular. In MicroPort ICDs, the discrimination algorithms work continiously, also during the persistence, which is why long persistence counters greatly reduce inappropriate therapies in case of supraventricular arrhythmias.
The menu showing the possible options for persistence in the VT zone:
Here is a figure going in depth of the working of the persistence counter in this case:

The persistence counter starts every time when the VT/VF counter is filled and starts at a value of 1. As we can see in this figure, the persistence counter is reset to 0 when the diagnosis is n longer VT (but SVT/ST in thise case). The persistence counter restarts at 1 when the diagnosis of VT (VTLC 3) is again made. Interestingly, there is a short interruption of the VT. While the VT counter remains filled (meeting the 6/8 criterium), the persistence counter is frozen (+0) until there are new events in the VT zone (+1). In this case, the persistence counter needed to reach 30 before the first treatment is launched (ATP in this case).