73-year-old male implanted with a secondary-prevention, dual-chamber defibrillator for ischaemic cardiomyopathy with sustained VT 8 years ago; box change with implantation of a Teligen defibrillator; multiple episodes of non-sustained VT or VF requiring 1 to 2 ATP sequences noted during a routine consultation
Summary
initially, the episode is classified in the VF zone
ATP is delivered, the shock is diverted due to reconfirmation failure
a second episode is diagnosed in the VT zone; a burst of ATP is delivered
EGM layout
AP-Sr VP-Sr cycle (Sr for sensor, meaning that the rate is set by the sensor: rate response)
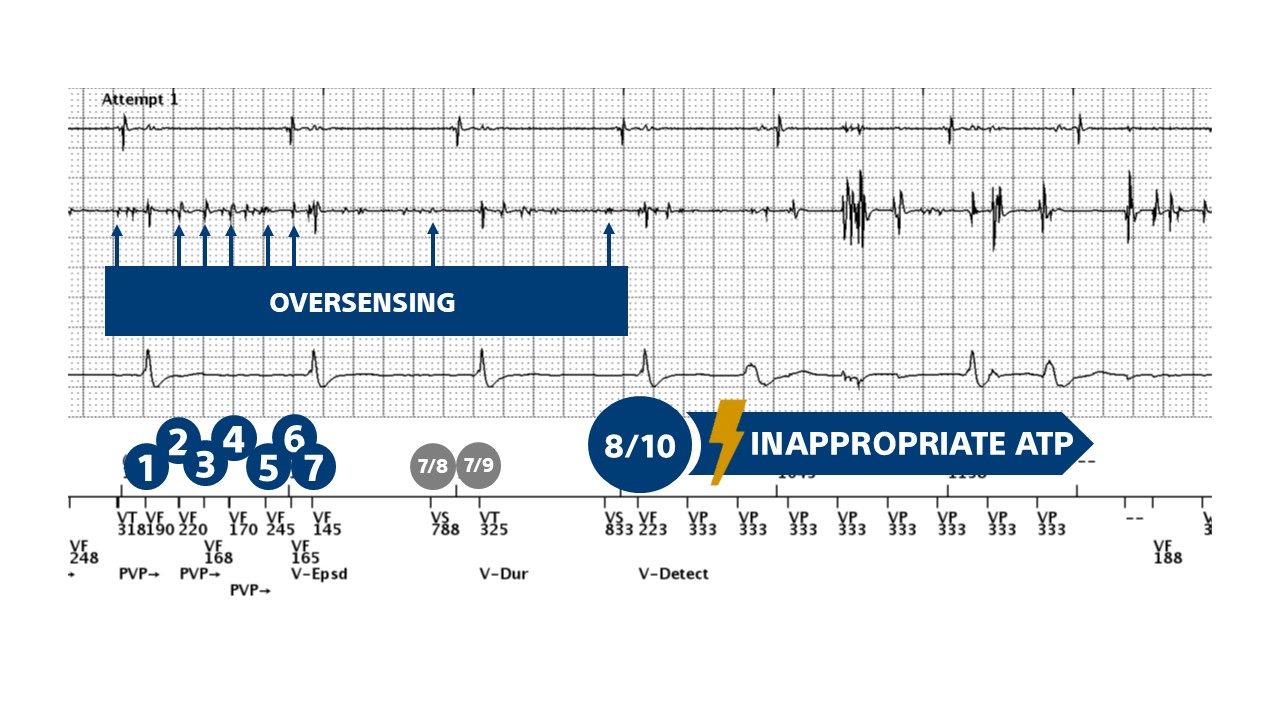
oversensing by the ventricular channel with signals of variable amplitude and morphology in the VT or VF zone; the shock channel shows no oversensing and allows differentiation of spontaneous ventricular activity; atrial pacing is at the sensor indicated rate ; the atrial rate is variable because it is influenced by ventricular oversensing
VF counter is filled (V-Epsd)
oversensing is intermittent and at the end of the duration, the rhythm is considered sinus; no therapy is delivered
new ventricular oversensing
the VF counter is filled and at the end of the duration, the first therapy is delivered.
during ATP (Quick Convert), ventricular capture is intermittent (2 effective stimuli, 6 ineffective stimuli)
oversensing continues following ATP and capacitor charging begins (the first cycle following the ATP sequence is not counted; 2 out of 3 cycles are then classified as VT or VF, explaining the start of capacitor charging).
when oversensing stops, the charge is diverted (the 6/10 rapid cycle criterion is no longer met)
resumption of oversensing
VT counter filled (V-Detect)
an ATP sequence is delivered; ventricular stimuli do not capture
Take home message
this tracing shows an example of inappropriate therapy due to lead dysfunction; a very rapid pacing sequence is delivered, illustrating one of the potential risks of systematically programming a pacing sequence for rates up to 300 beats/minute; for these very high heart rates, there is an increased risk of inappropriate treatment by rapid pacing of non-physiological, false-positive tachycardias (lead fracture, oversensing of P, R or T wave, electromagnetic interference)
in patients with ischemic cardiomyopathy, VT can be triggered by a rapid ventricular pacing protocol; this perfectly explains the potential pro-arrhythmogenic effect of inappropriate anti-tachycardia pacing , particularly when the pacing protocol is very aggressive in the VF zone; the pro-arrhythmogenic risk has been particularly well documented for anti-tachycardia pacing and for low-amplitude shocks (much more so than for maximum-amplitude shocks, which are less arrhythmogenic)
in this example, the pro-arrhythmogenic risk is reduced, since ventricular capture is not always effective due to the lead dysfunction
there is now a consensus favoring treatment with anti-tachycardia pacing over shocks for organized ventricular arrhythmias; in fact, many episodes diagnosed as VF by the defibrillator on the basis of a rate > 200 beats/minute correspond to rapid monomorphic VT, which can be effectively treated by pacing; anti-tachycardia pacing is painless and reduces battery consumption and should therefore be the preferred first-line treatment for organized ventricular arrhythmias, even when they are very rapid
on the other hand, systematic programming of anti-tachycardia pacing for rates of up to 300 beats/minute has not been shown to be effective and carries a pro-arrhythmogenic risk if the therapy is inappropriate
This figure shows overdetection and rapid ventricular pacing in the VF zone with intermittent capture.