male with dilated cardiomyopathy and numerous episodes of non-sustained VT; implanted with a Resonate triple-chamber defibrillator
Summary
episode classified as non-sustained VT
EGM layout
spontaneous rhythm in the atrium and biventricular pacing
onset of ventricular tachycardia (regular, monomorphic with atrioventricular dissociation)
alternation between a cycle classified in the VT zone and a cycle classified as an extrasystole; to trigger the search for the 8/10 criterion, 3 consecutive cycles in a tachycardia zone are required; this first VT cycle (followed by a cycle sensed outside a tachycardia zone) therefore does not count towards the 8/10 criterion.
third consecutive cycle in the VT zone (3 consecutive cycles criterion met)
VT episode (V-Epsd) after 8 cycles in VT zone (including 3 consecutive cycles); start of initial VT zone duration (programmed to 12 seconds)
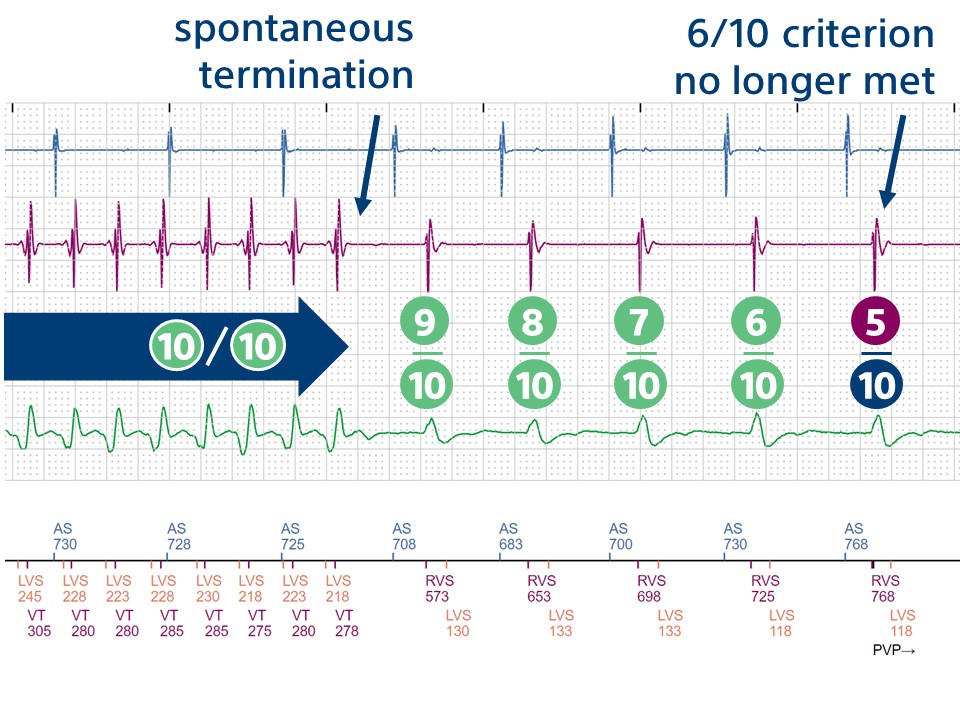
spontaneous termination
after 5 cycles outside the tachycardia zone, criterion 6/10 is no longer met
end-of-episode marker (10 seconds after criterion 6/10 is no longer met)
Take home message
this patient had multiple episodes of non-sustained VT prior to implantation; the priority during programming is to avoid any therapy on these spontaneously resolving arrhythmia episodes; 2 options may be preferred: programming lower limits of tachycardia zones above the rate of clinical VT, or programming initial durations long enough to promote spontaneous termination
this trace illustrates one of the major developments in the programming of implantable defibrillators, namely the programming of longer initial durations; one of the main programming objectives of the first implanted devices was to treat the various arrhythmias detected (VT or VF) without delay; there are several explanations for this initial strategy and tendency towards rapid treatment with a device-based shock: 1. most initial patients received implants for secondary prevention, 2. there was concern surrounding the risk of VF undersensing , 3. various studies had shown a positive correlation between monophasic shock defibrillation threshold and the duration of the episode; similarly, documentation of inappropriate therapies was limited since the very first devices did not record tracings
various technological advances, an increase in the proportion of patients implanted for primary prevention, widely publicized problems of inappropriate therapies due to lead dysfunction, and the results of various large-scale studies have all contributed to a considerable change in the way modern defibrillators are programmed: the PREPARE study was the first to show that longer detection times could reduce the number of shocks delivered without increasing complications (syncope, sudden death, etc.); the Multicenter Automatic Defibrillator Implantation Trial: Reduce Inappropriate Therapy (MADIT-RIT) showed the positive impact of programming a single VF zone (> 200 beats/minute) or implementing delayed therapy (1 minute for the zone between 170 and 200 beats/minute and 12 seconds between 200 and 250 beats/minute) compared to conventional programming; other studies and meta-analyses have confirmed benefits in terms of reducing appropriate or inappropriate therapy and reducing mortality, suggesting a definite benefit to such programming.
the nominal programming suggested by manufacturers has gradually evolved; in 2015 and again in 2019, consensus guidelines for the programming of implantable defibrillators reiterated the need for default programming of high detection zones with longer initial durations
for a patient implanted with a Boston ScientificTM defibrillator for primary prevention, 2 programming options can be selected: 1) delayed therapies: a VT zone from 185 beats/minute with an initial duration of 12 seconds and a VF zone from 250 beats/minute with an initial duration of 5 seconds; 2) therapies with a higher detection zone: a single VF zone from 200 beats/minute with an initial duration of 2.5 seconds.
for a patient implanted with a Boston ScientificTM defibrillator for secondary prevention, it is recommended to add a VT zone (VT-1 if delayed therapies are chosen) at a rate 10 to 20 beats slower than the clinical tachycardia, with an initial duration of at least 12 seconds.
as this patient’s clinical VT was relatively rapid (oscillating around 200 beats/minute), the longer initial duration option (12 seconds for the VT zone, 5 seconds in the VF zone) was preferred
this trace also provides details of how detection works; initially, 3 consecutive fast ventricular cycles (VT-1, VT or VF) must be detected for the device to search for the existence of an episode (these 3 consecutive cycles are then included in the search for criterion 8/10); throughout the duration, criterion 6/10 rapid cycles must be maintained; on this trace, the arrhythmia terminates and after 5 slow cycles, the duration is interrupted; 10 seconds later, the end-of-episode marker appears (non-programmable criterion; criterion 8/10 not verified 10 seconds after an untreated or ATP-treated episode, 30 seconds after a shock).
This figure shows the spontaneous termination and the point at which the 6/10 criterion is no longer met.