75-year-old male with ischemic cardiomyopathy; implanted with a Resonate triple-chamber defibrillator
Summary
episode classified in the VF zone
5 maximum amplitude shocks
EGM layout
possible slow VT
acceleration of arrhythmia into the VF zone
end of duration and start of capacitor charging
arrhythmia degenerates into VF (very rapid, disorganized ventricular activity)
end of charge and 41 Joule electric shock delivered on the second fast cycle (synchronized to the R wave)
reinitiation of an organized arrhythmia
redetection criterion 8/10 verified (start of redetection time for VF zone)
end of 1 second duration and charging of capacitors
shock delivered at end of charge after the 500 ms post-shock window (no need to validate the 2/3 rapid cycle criterion)
reinitiation of ventricular arrhythmia
redetection criterion 8/10 verified (start of redetection time for VF zone)
end of 1 second duration and charging of capacitors
shock delivered at end of charge after 500 ms post-shock window (no need to validate the 2/3 rapid cycle criterion)
fourth shock
fifth shock
arrhythmia terminatio
Take home message
the patient has a high defibrillation threshold, and five shocks are required to permanently disrupt the VF episode
even though technological advances have significantly improved a defibrillator’s ability to terminate VF episodes (95% of patients now have a sufficient safety margin), an increase in the number of patients implanted necessarily increases the number of patients with a high threshold.
the existence of a high defibrillation threshold is the result of a complex interaction between molecular, electrical, mechanical, anatomical, neurohumoral or pharmacological factors
all initial major studies demonstrating a beneficial effect to defibrillator implantation for improving survival, included in their protocols a defibrillation test at the time of implantation to verify proper device function
following the results of randomized trials, defibrillation threshold assessment at the end of implantation is no longer routinely performed; however, the presence of specific risk factors may result in this test being performed in certain patients suspected of having an insufficient safety margin (right-sided implantation, suspicion of lead dysfunction, atypical position of the defibrillation lead, patient on amiodarone, obese patient, etc.).
the detection of an elevated defibrillation threshold during a spontaneous episode of VF constitutes an absolute emergency, and should lead to management aimed at 1) reducing the risk of arrhythmia recurrence, 2) identifying reversible causes (hypomagnesemia, hypocalcemia, hyperkalemia, acidosis, pneumothorax, pleural effusion, tamponade…) contributing to the increased threshold, and 3) optimizing the defibrillation circuit (lead position, box, number of coils available, programmable parameters, etc.).
to optimize shock wave characteristics, some parameters are programmable, while others are not, depending on the manufacturer; in a Boston Scientific defibrillator, shock amplitude, vector and polarity are programmable.
the key parameters for successful defibrillation are the voltage and duration of shock delivery; shock impedance corresponds to the sum of the forces opposing defibrillation current output in the box-lead-myocardial tissue circuit; increased impedance limits the amount of energy delivered and helps raise the defibrillation threshold
in a monophasic shock, the polarity of each electrode does not vary during the shock, whereas it reverses when the shock is biphasic; the shape of the shock wave is necessarily biphasic for a Boston Scientific defibrillator; the first phase of a biphasic shock is equivalent to that of a monophasic shock, albeit with less critical mass ; the second phase brings the membrane potential as close as possible to zero, to avoid reinduction of tachycardia or ventricular fibrillation; while early devices delivered monophasic shocks, the introduction of biphasic shocks on modern platforms has significantly reduced defibrillation thresholds and the risk of immediate reinduction
tilt corresponds to the terminal voltage at which polarity is reversed during a biphasic shock and is not programmable for a Boston Scientific defibrillator (tilt 80%); phase 1 is truncated when the initial peak voltage has decreased by 60% (residual voltage 100%-60%=40%); phase 2 is truncated when the peak voltage (corresponding to the residual voltage of 40%) has decreased by 50% (40/2=20%); the pulse durations of the 2 phases are not programmable and are a consequence of tilt and shock impedance; the energy delivered is always lower than the energy charged (generally around 14% lower).
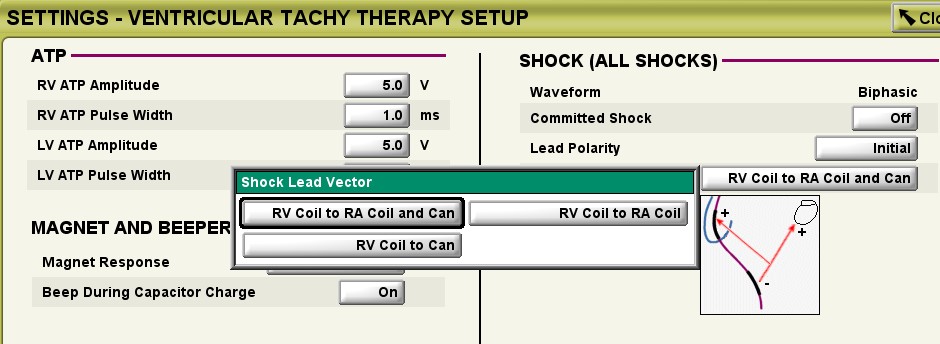
the shock vector can be modified when the implanted lead is dual-coil; when the lead is single-coil, the only vector available is that between the right ventricular coil and the can, the can always being active and an integral part of the defibrillation circuit; when the lead is a dual-coil lead, 3 options are programmable: single-coil (right ventricular coil – can), dual-coil (right ventricular coil – can + superior vena cava coil), cold can (right ventricular coil – superior vena cava coil).
nominal shock polarity programming varies from one manufacturer to another; a meta-analysis suggested that a configuration using the right ventricular coil as the anode for the first phase (so-called anodic shock) enabled a certain number of patients to achieve a better defibrillation threshold than a cathodic shock (inverted configuration), with a lower risk of induction; for a Boston Scientific defibrillator, in nominal mode, the first shocks have a cathodic polarity (initial = RV coil as cathode during the first phase, then reversed for the second); the polarity of the last shock in the series is necessarily reversed compared with that of the 7 preceding shocks; it may therefore be desirable to reverse the polarity for the first shocks in this patient with a high threshold
lead repositioning, implantation of a double-coil lead, addition of a coil in the azygos vein, coronary sinus or pericardial space may be options to modify the defibrillation vector
For a dual coil lead, there are 6 configuration options by varying the polarity and shock vector:
Vector
RV coil to RA coil and can: this vector is also known as vector V-TRIAD (double coil); the can serves as an active electrode («active can») in association with the double coil defibrillation lead; energy is delivered simultaneously from the distal coil to the proximal coil and from the distal coil to the can
RV coil to can: this vector also uses the can as an active electrode («active can», simple coil); energy is only delivered from the distal coil to the pulse generator can.
RV coil to RA coil: this vector, also known as the «cold can», cancels out the use of the box as an active electrode; energy is sent from the distal to the proximal coil.
Polarity
Initial polarity: the right ventricular coil is negative for the first phase (cathode), the casing and/or the superior vena cava coil are positive (anode); this corresponds to a cathodic shock.
Reversed polarity: the right ventricular coil is positive for the first phase (anode), while the casing and/or superior vena cava coil are negative (cathode); this corresponds to an anodic shock.
The RV coil to can configuration is the only effective configuration for a single-coil lead: the other 2 configurations must not be programmed; for the RV coil to RA coil configuration, no shock would be delivered; this vector must therefore never be used with a single-coil lead; when programmed, a warning window appears requesting verification that the lead is indeed double-coil.