80-year-old male implanted with an Incepta CRT defibrillator
Summary
episode classified in the VT zone
4 bursts + 3 ramps + 1 shock of 11 Joules + 1 shock of 41 Joules
EGM layout
regular monomorphic ventricular tachycardia (atrioventricular dissociation) diagnosed in the VT zone
burst of 8 complexes at fixed rate; biventricular pacing
ineffective burst and ongoing arrhythmia
second burst with additional paced impulse
third burst
fourth burst
first ramp
second ramp
third ramp
next therapy is a shock; capacitor charging begins
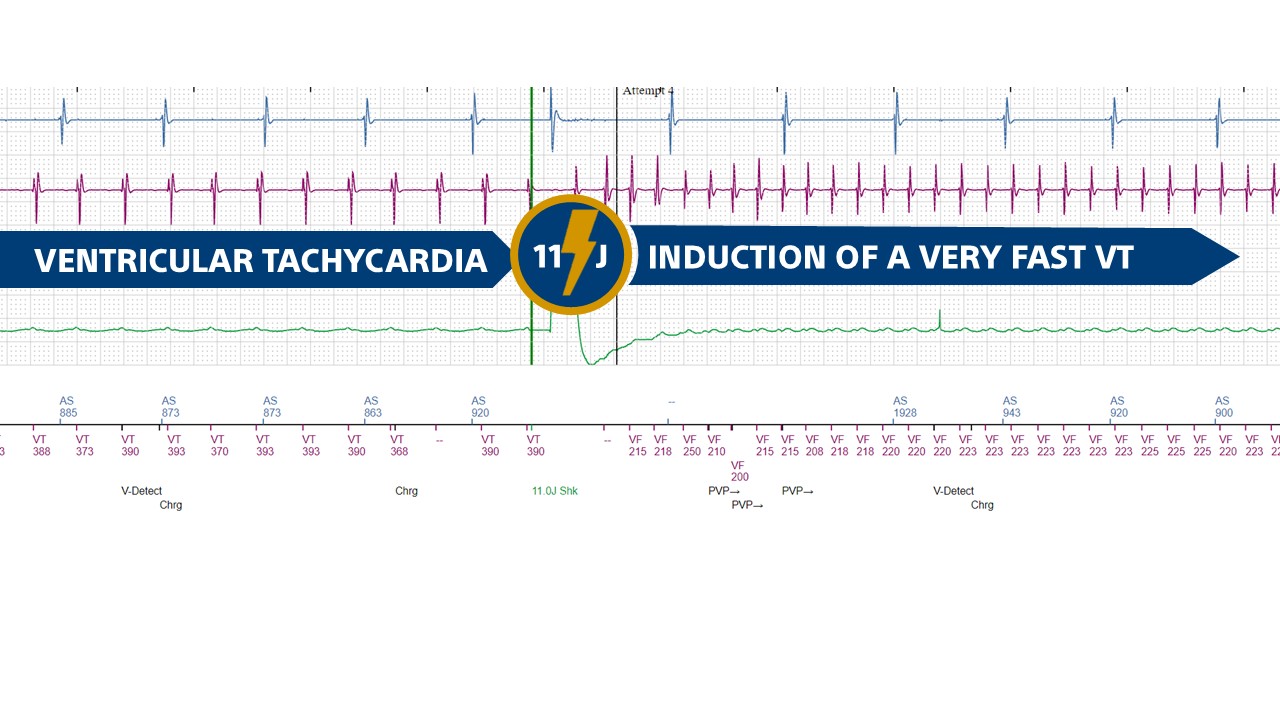
11 Joule shock delivered after the end of the diversion window on the second rapid ventricular cycle (2/3 rapid cycle criterion verified)
accelerated ventricular rate with very fast VT detected in the VF zone
VF episode detection and capacitor charging
41 Joule effective shock
Take home message
the amplitude of the first shock in the VT zone can be programmed at maximum energy or at a lower amplitude (in the order of 10 to 15 Joules)
there are a number of advantages to programming a first shock of moderate amplitude (10-15 Joules): 1) this amplitude is very often sufficient to terminate a VT episode; 2) the charge time for this amplitude is very short, even if the few seconds difference in comparison to a maximum amplitude shock may not be clinically important when the shock occurs after 3 burst +/- 3 ramp sequences (more than one minute of arrhythmia); 3) power consumption is lower for a shock at 10 Joules versus 41 Joules, even if battery usage is only slightly affected if a limited number of shocks are delivered; 4) even though for most VT episodes the shock is delivered while the patient is still conscious, the painful nature of the shock contributes minimally to decision-making regarding the amplitude of the first shock, since it is difficult to demonstrate a direct relationship between the amplitude of the shock delivered and the amplitude of the pain caused; 5) various studies have demonstrated the deleterious nature of an electric shock and its association with an adverse prognosis ; it therefore seems logical to think that a 10-15 Joule shock will have fewer negative consequences than a 41 Joule shock, and it seems advisable to choose the least traumatic therapy possible.
this tracing shows the main drawback of programming a low-amplitude shock (11 Joules) in the VT zone: pro-arrhythmogenic risk and acceleration of the arrhythmia (concept of upper limit of vulnerability); in this patient, the shock has the opposite effect to what was intended; below a certain value, which varies according to the patient and is directly linked to the defibrillation «threshold», not only can a shock prove ineffective in terminating an arrhythmia, but it can also accelerate and cause degeneration of a monomorphic VT into a polymorphic arrhythmia, compromising the patient’s short-term prognosis.
This figure shows how a medium-amplitude shock accelerates a monomorphic VT at 160 beats/minute into a very rapid ventricular flutter.