Long VT
Patient
A 50-year old patient with dilated cardiomyopathy with commonly well tolerated VTs comes in for a regular device check.
The newest episode with therapy is the following:
Trace
Interval plot
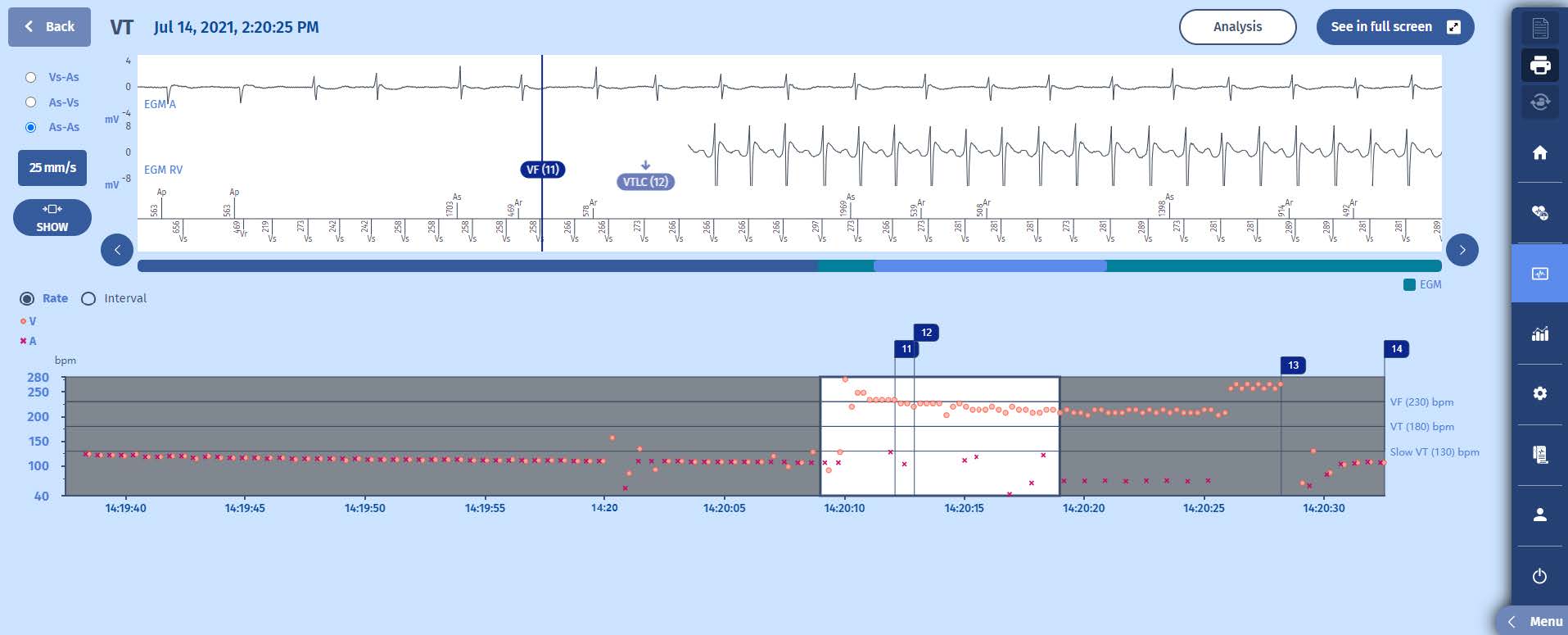
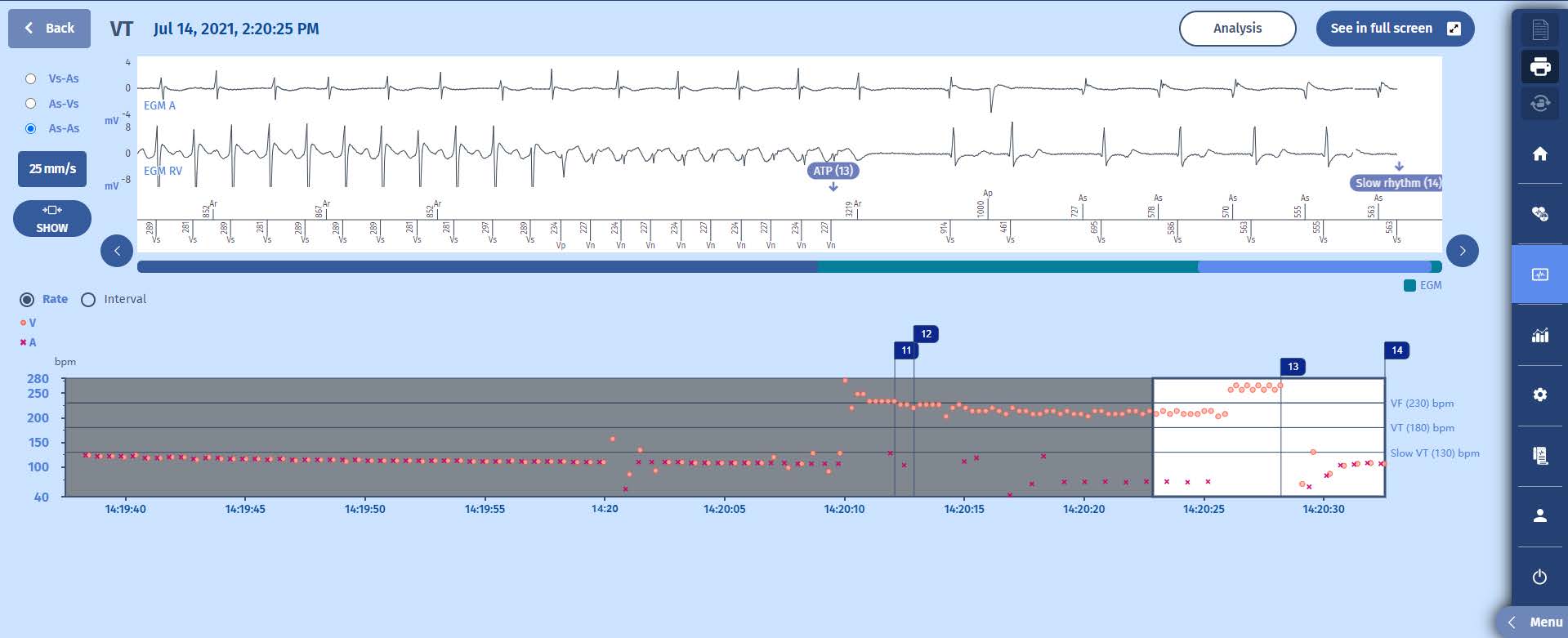
The episode begins with an elevated heartrate at around 110 beats per minute. There are multiple ventricular events with a shorter cycle, suggesting the existence of PVCs. There is a sudden acceleration of the ventricular rhythm into the VF zone but the arrhythmia stabilizes in the VT zone. After a period of 15 seconds of stable VT in the VT zone, an ATP is delivered, which terminates the arrhythmia. The last marker indicates filling of the “return to slow” counter, which means the end of the episode.
EGM
1 At the beginning of the episode we see atrial pacing at 100-110/min with preserved atrioventricular conduction.
2 Suddenly there are rapid ventricular events which fill the VF counter, marker VF (11)
3 The ventricular events slow down and the VT counter is filled shortly after.
4 At this marker, VTLC (12), the persistence counter steadily increases with each ventricular event.
5 When the persistence counter is filled (50) after 15 seconds, an ATP is delivered
6 The ATP terminates the VT
Comments
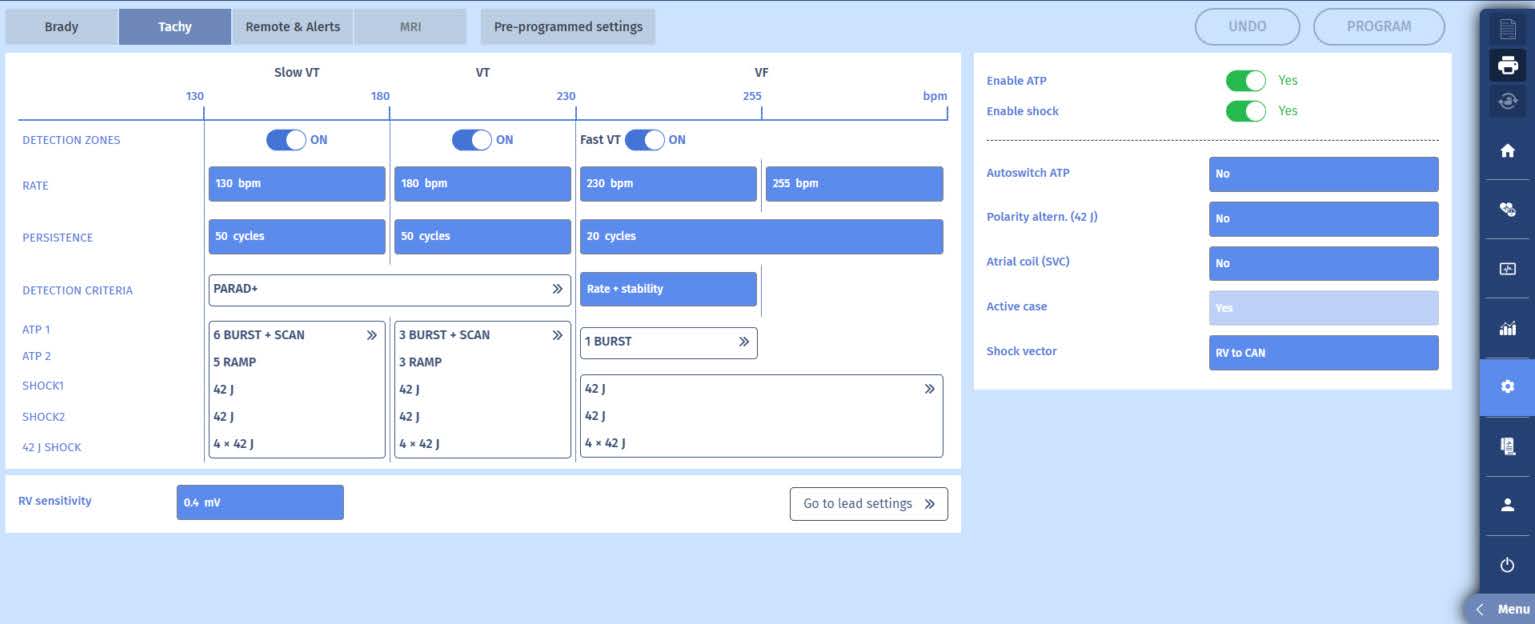
This episode shows correct sensing of a VT, terminated by a single burst. There is a substantial delay before the ATP is delivered which is caused by programming of a long persistence counter (at 50). This was decided after the patient had many nonsustained VTs which were well tolerated. Many of the VTs which are treated after a persistence counter of 20 or 30 could actually self terminate. This way there is no delivery of ATP, which is associated with a small risk of accelerating the rhythm into a faster VT or even VF, which would be more symptomatic and even dangerous for the patient. Up until a decade ago ICDs were programmed aggressively, making sure that VT and VF was quickly treated. The idea was to protect the patient from the deleterious effects of
persisting VT or VF, which may degrade and become more symptomatic and harder to treat (risk of non-effective shocks). This dogma has been resolved by the publication of multiple studies (such as MADIT-RIT and Painfree) which show the deleterious effects of early treatment of VT due to dangerous side effects of ATP (acceleration) and shocks (which are harmfull to the heart).
Take home message
When patients have many occurrences of VT and which suffer from the many treatments(ATP/shocks), it may be decided to program a longer persistence to allow for the VT to
self terminate. For this patient this has lead to significant less treatments, but not all VTs self-terminated, as evidenced by this episode. It was agreed with the patient to keep the current programming.

