A 68-year old patient with ischemic cardiomyopathy has been implanted with a dual chamber ICD (Platinium DR). He presents for a routine check-up. He claims not to have any symptomes
and not to have felt any ICD shocks.
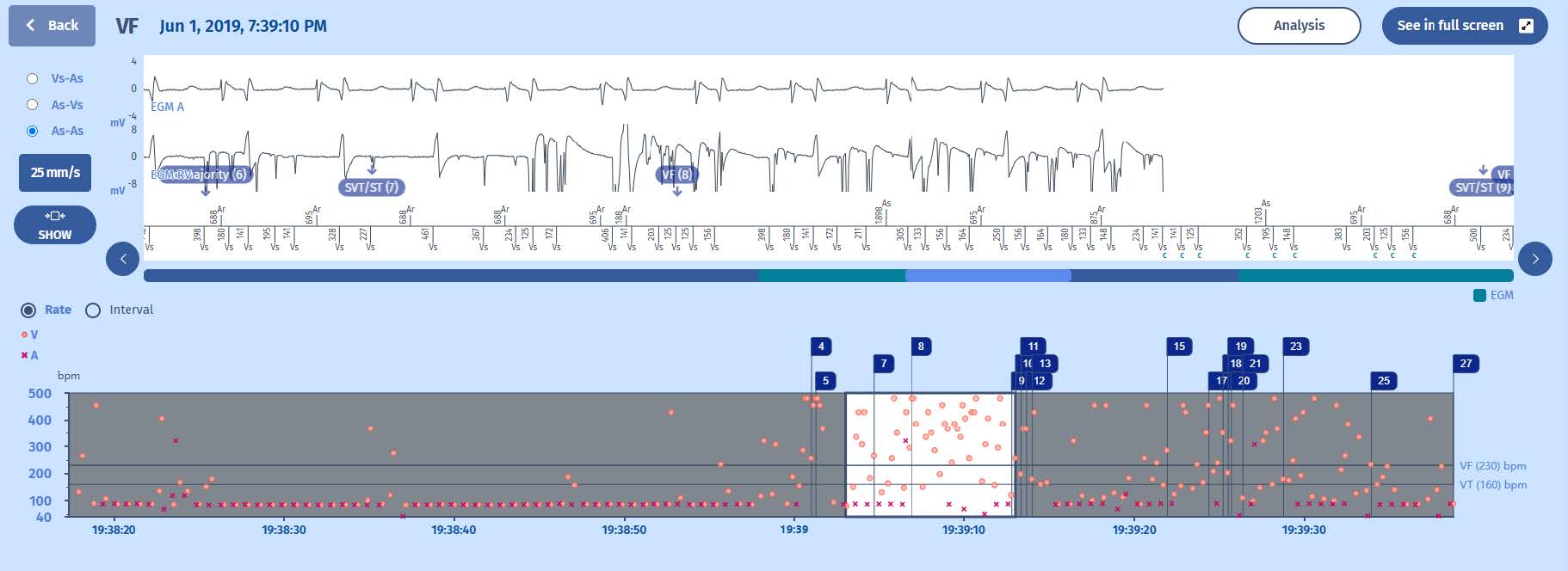
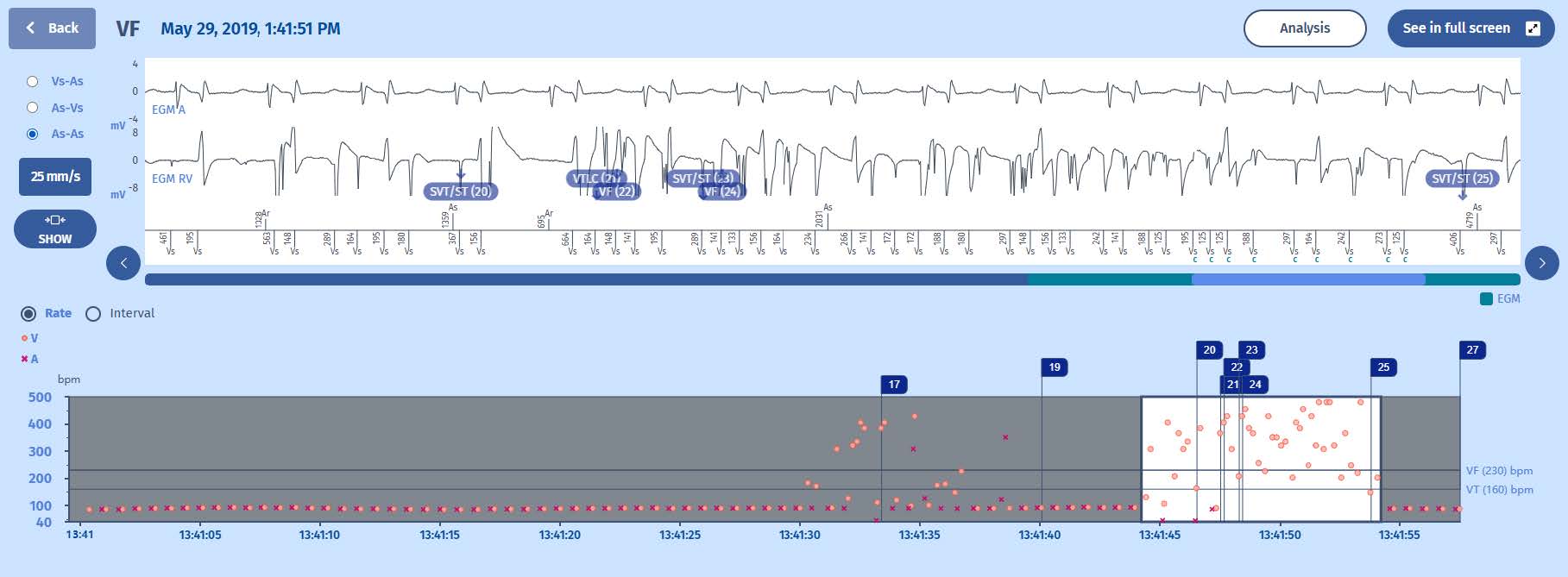
Programmer Screen
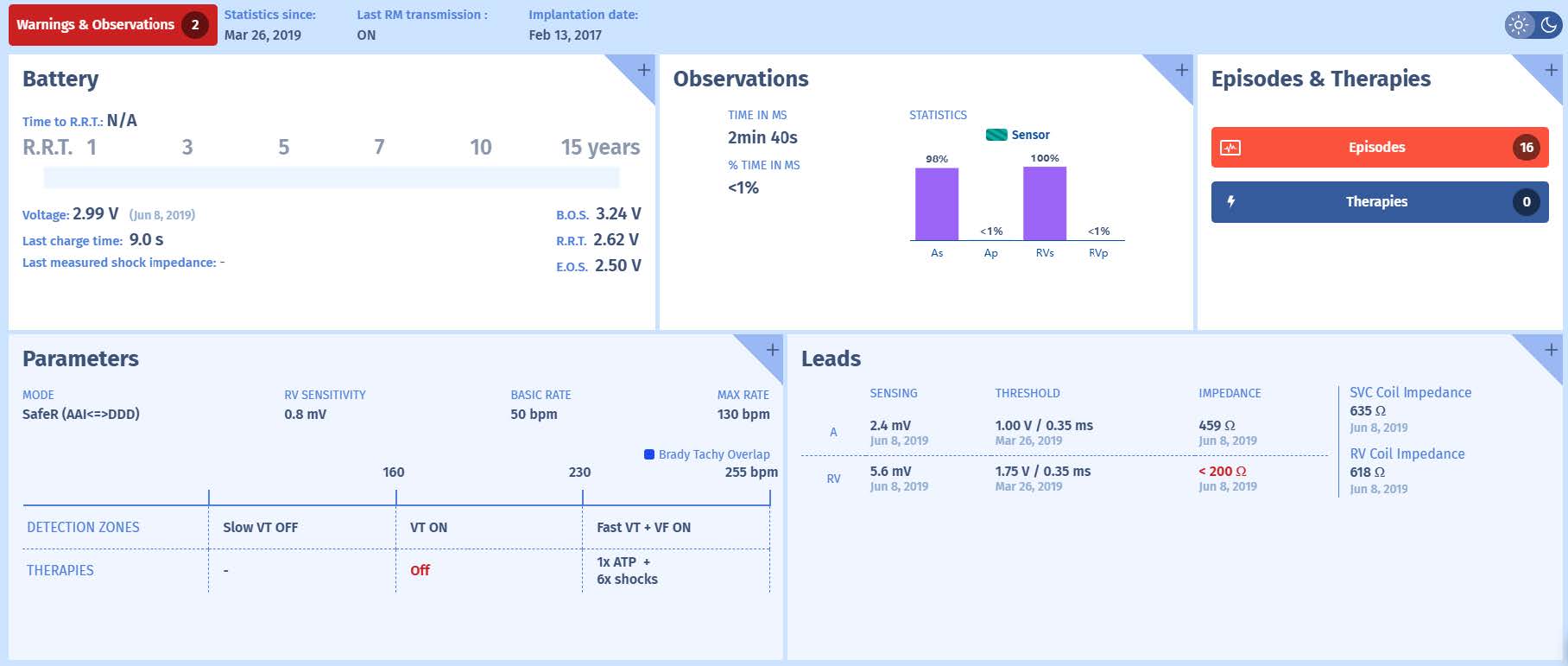
Warning screen

Luckily for the patient, the noise is intermittent and stops before the delivery of inappropriate therapies. Preventing inappropriate therapies in case of lead failure is a priority for the
ICD companies. The combination of programming changes (extending counters, activating discriminators, activating dedicated algorithms) and remote monitoring (examination of nonsustainedepisodes, non-treated sustained episodes, impedance changes) have resulted in asignificant decline in inappropriate therapies for lead failure. When lead failure is suspected,
certain maneuvers may exacerbate lead noise to confirm the diagnosis. Examples are arm movements, deep breathing and pocket manipulation (certainly in case of insulation breach). A
chest X-ray is often performed which may reveal lead fracture but can also serve for planning of the lead extraction or lead implantation procedure. When lead failure has been confirmed,
ICD therapies need to be deactivated and in case of pacemaker dependency; the pacemaker programmed accordingly (for example asynchronous pacing in VOO mode to avoid inappropriate
inhibition). Then within a short delay, a new lead should be implanted while abandoning or whenpossible, extracting the faulty lead.