Fast tachycardia accelerated by therapy
Patient
A 66-year-old man implanted with Platinium DR for dilated ischemic heart disease without prior infarction and ejection fraction of 28%, narrow QRS, in secondary prevention. Follow-up control. Asymptomatic patient.
Device interrogation

EGM
Discussion
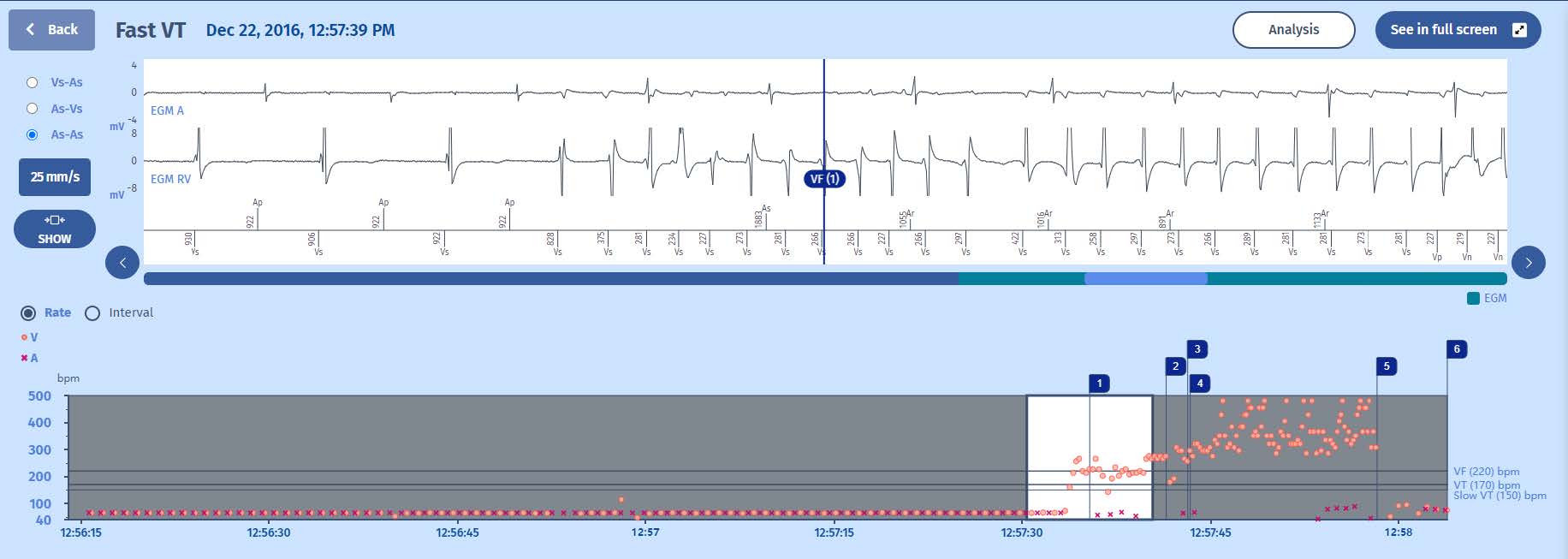
This example explains the sequence of therapies in the FVT/VF zone.
1 The tachycardia is immediately detected in the VF zone after 8 tachycardia cycles. We can see that the tachycardia is not stable at the outset
2 A persistence of 16 cycles is therefore triggered at the end of which
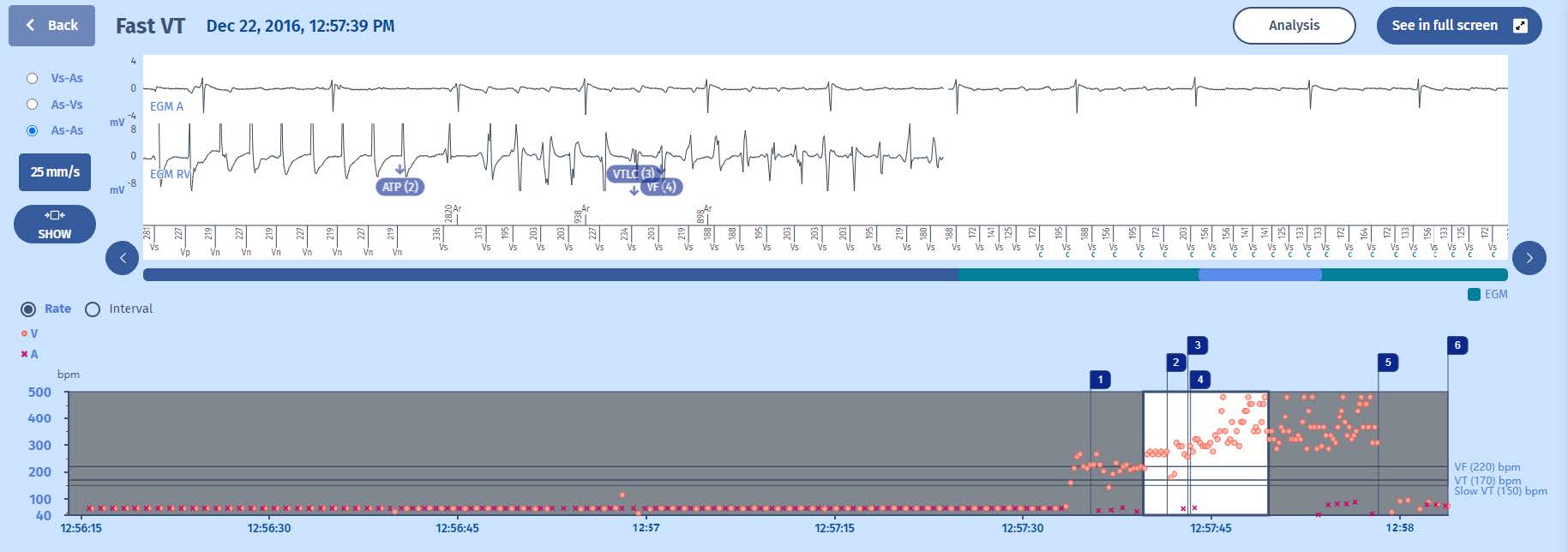
3 the first therapy in the FVT zone is initiated since the tachycardia is still in the VF zone at the end of the persistence with a stable rhythm: the therapy delivered is an 8-cycle burst
4 This degrades the tachycardia into a ventricular fibrillation, first observed in the VT zone (VTLC marker) since the first two cycles after the ATP are longer and diagnosed as VF in the next cycle (VF marker), hence a new persistence of 16 cycles is triggered.
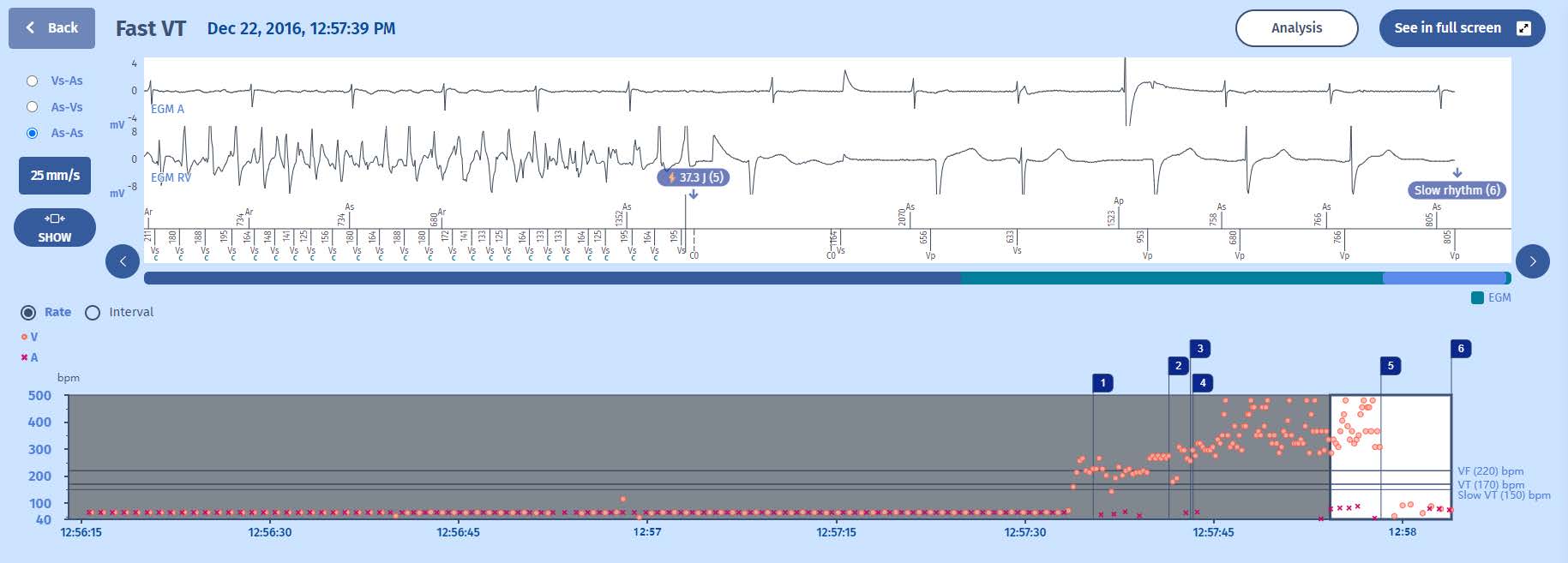
5 The second line of therapy consists in shocks, hence the charge of the capacitors.
6 The VF continued throughout the charge, the device was able to confirm the charge cycle-to-cycle, and at the end of the charge, a 195 ms cycle confirms that the VF continues, and thus a shock is delivered (37.3 J).
7 The first signal after the shock is the opening of the detection chains (for the implant, the coupling interval of this cycle is 164 ms: the post-shock interval is 1164ms that quals the one-second blanking period plus 164 ms), the ensuing 6 cycles are slow
which terminate the episode.
Comments
Here we have the example of a burst causing the degradation of a fast ventricular tachycardia into a VF and which requires a shock. This tachycardia is fast and rather unstable at the outset. One can therefore raise the question of programming a longer persistence duration to allow the tachycardia the opportunity to terminate spontaneously before the response of the defibrillator. The programmed persistence in the VF zone is 16 cycles. An increase in the number of persistence cycles should therefore be discussed.
Take home message
An ATP burst in the VF zone can allow terminating the rhythm disorder without the need for a defibrillation shock at the outset.
The programming of a long persistence duration is recommended to allow the tachycardia to terminate spontaneously without defibrillator intervention.

