- these 2 traces illustrate the complexity of defibrillator programming; in the first trace, 1/1 atrial tachycardia is poorly discriminated by the Onset/Stability algorithm; in fact, the atrial rate exceeds the AF threshold and the rhythm is stable; the device suspects a possible dual tachycardia and delivers a burst of anti-tachycardia pacing which terminates the atrial arrhythmia; it is therefore an inappropriate therapy that has a beneficial effect; this type of 1/1 atrial tachycardia is almost systematically poorly discriminated by this algorithm, therefore a decision was made to switch to the Rhythm ID option, since the morphology criterion is theoretically effective in this type of tachycardia
- the second plot shows that an identical episode of tachycardia (1/1 atrial tachycardia) that is then correctly discriminated in this patient with inhibition of therapies; the episode ends spontaneously, which raises the question of reprogramming the initial duration (lengthening it significantly) in the VT zone so as to maximize the probability of spontaneous termination without intervention of the discrimination algorithm; another option is to increase the lower limit of the VT zone (to 200 beats/minute for example), so as to avoid any overlap between the rates of this atrial tachycardia and the rates of possible VT.
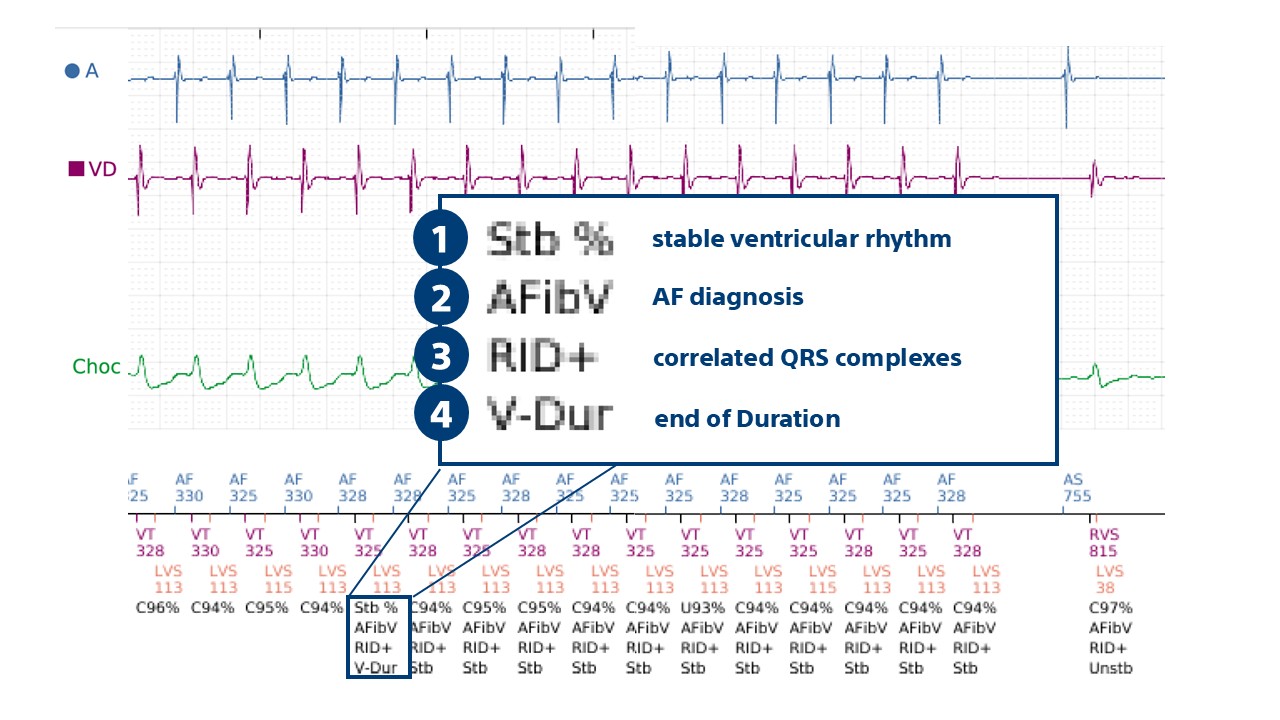
On the second trace:
– the rhythm is stable with a diagnosis of AF: this would therefore lead to a diagnosis of VT if the Onset/Stability algorithm had been programmed
– QRS complexes are correlated (RID+), which explains why therapies are inhibited