Dual-chamber discrimination, atrial refractory periods and V>A criterion
Patient
- 66-year-old male with severe ischemic cardiomyopathy; implanted with a dual-chamber defibrillator
Summary
- initial diagnosis of supraventricular tachycardia based on Rhythm ID with no treatment
- subsequent diagnosis of a VT with a series of 5 ATP bursts
EGM layout
- probable sinus tachycardia with 1/1 AV relationship; alternating cycles classified as VS and VT-1
- criterion 8/10 met
- at the end of the duration, no therapy is delivered; the rhythm is stable and the tachycardia vectors are correlated with the reference vector.
- ongoing cycle-by-cycle analysis
- probable variation in the time at which the R wave is detected by the ventricular lead, explaining the variability of ventricular intervals; rhythm considered unstable; vectors remain correlated, no therapy delivered
- Stability criterion met again
- probable atrial extrasystole with some irregularity to the rhythm
- new atrial extrasystole; as the PR is relatively long, the atrial extrasystole occurs at the same time as ventricular sensing of the R wave; it falls within the atrial refractory period after ventricular sensing and is not sensed.
- since the atrial extrasystole is not counted, the subsequent compensatory rest is responsible for a false slowing of the atrial rhythm compared to the ventricular rhythm; V>A criterion is satisfied (comparison of atrial and ventricular rate over the previous 10 cycles); this criterion takes precedence over all others; decision to treat
- first ATP burst
- continuation of sinus tachycardia
- second ATP burst
- third ATP burst
- fourth ATP burst
- fifth ATP burst
- slowing of sinus rate below VT-1 zone and end of episode
Take home message
- this episode corresponds to a sinus tachycardia that was initially discriminated correctly; when the vectors are correlated, the device inhibits therapies
- the device is deceived during a second phase by the non-sensed atrial extrasystole that falls in the refractory period; in fact, the V>A criterion takes precedence over all other criteria, including morphology analysis
- as a general rule, the V>A criterion enables correct classification of the majority of ventricular tachycardias (atrioventricular dissociation is found in at least 80% of VTs); implementation of this criterion implies good atrial sensing; when the patient has imperfect atrial sensing (small amplitude signals or functional under- sensing, with atrial signals falling in the refractory period), this criterion, which takes precedence over other discriminants (morphology, stability, etc), systematically leads to a diagnosis of VT and must therefore be deprogrammed.
- for this patient, a first solution could be to avoid overlap between the detection/treatment zones and faster physiological rates
- another option is to preferentially use discrimination based on vector analysis, which seems perfectly suited to this patient; this involves deprogramming the V>A criterion responsible for the inappropriate therapies.
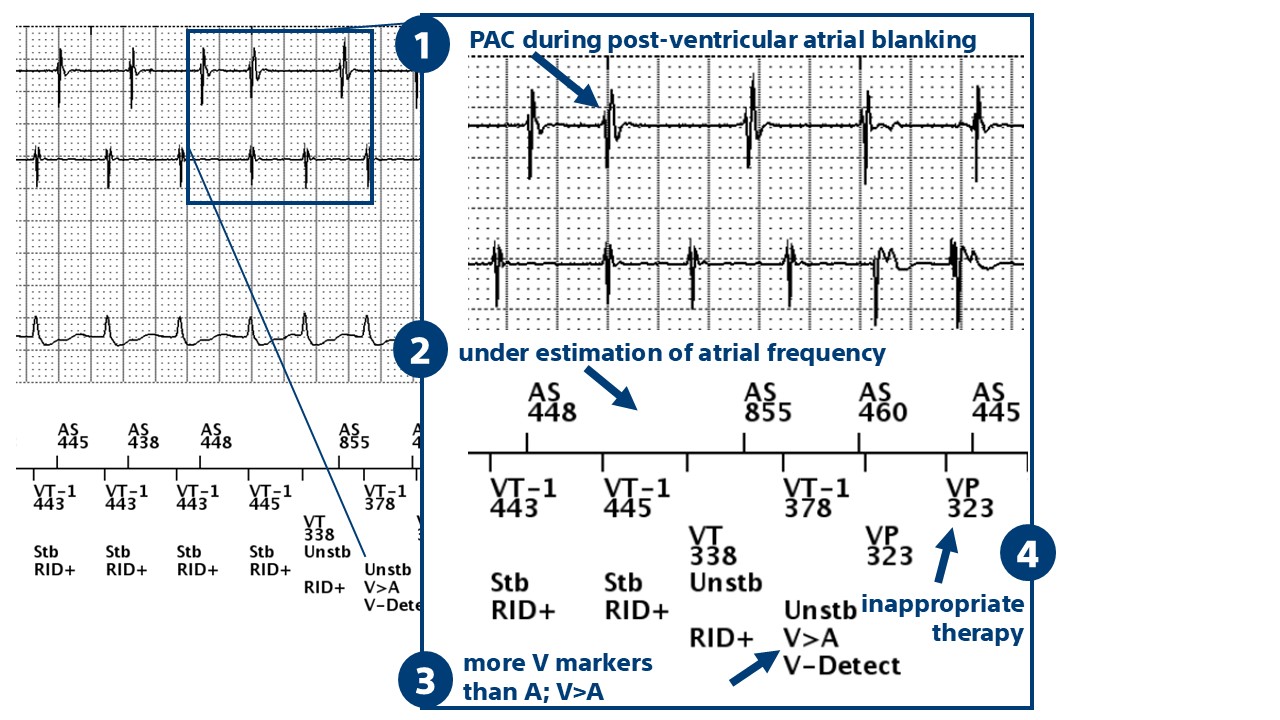
On this tracing, we can see that the morphology analysis is in favor of SVT (RID+); an atrial extrasystole falls into the post-ventricular atrial blanking, is not sensed and distorts the atrial rate calculation; the V>A criterion is satisfied and inappropriate therapy is delivered (burst).

