

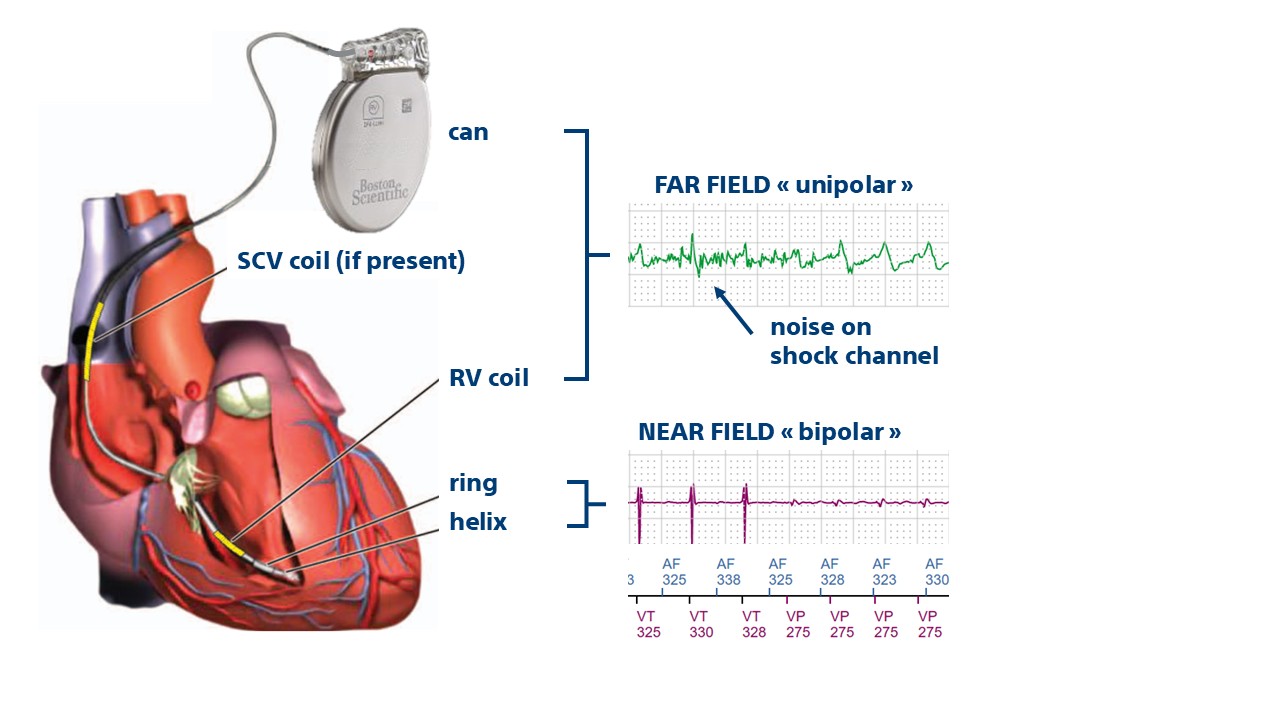
The shock channel is recorded between the RV coil and the defibrillator can located in the left pre-pectoral space; it is therefore a “unipolar” signal (only one electrode is located in the heart); this trace shows the poor quality on the shock channel signal due to oversensing of pectoral myopotentials which explains the lack of correlation with the reference ventriculogram and the occurrence of inappropriate therapies.