male with ischemic cardiomyopathy; implanted with a Resonate triple-chamber defibrillator
Summary
episode classified in the VF zone
41 joule shock with a charge time of approximately 10 seconds
76 Ohm shock impedance (single-coil lead)
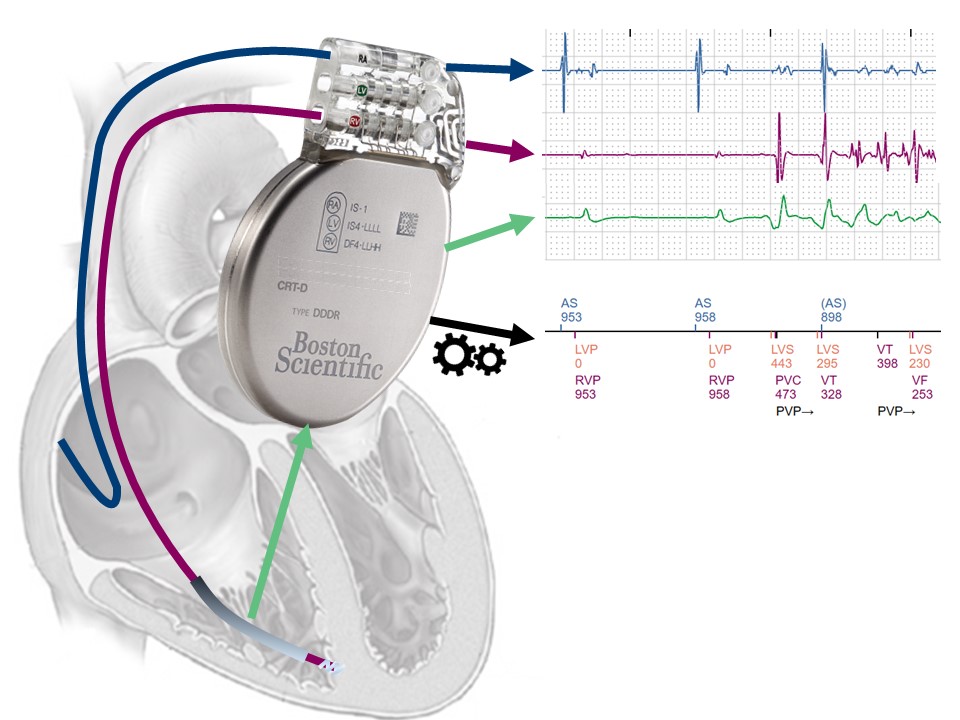
EGM layout
sinus rhythm and biventricular pacing (AS, RVP-LVP)
spontaneous, very rapid, polymorphic ventricular arrhythmia; the first 2 cycles are classified as VT, the following cycles as VF
V-Epsd marker; 8/10 criterion fulfilled for VT zone (2 cycles in VT zone + 6 cycles in VF zone); initial detection duration for VT zone starts on this beat
on this cycle, the initial detection window for the VF zone is satisfied (8 cycles in the VF zone); the initial detection duration for the VF zone begins on this beat; the VF zone duration takes precedence over the VT zone duration; even if the VT zone duration ends before the VF zone duration, if the 6/10 criterion is satisfied for the VF zone, the VT zone therapies are suspended until the VF zone duration ends.
persistence of arrhythmia detected in the VF zone for the initial duration of 5 seconds in the VF zone (V-Detect)
start of capacitor charging
ventricular sensing remains acceptable during charging, with the exception of a few under-sensed cycles explaining the VT markers; criterion 6 out of 10 remains fulfilled during charging.
end of charge; this charge lasted approximately 10 seconds, with the output of the pending shock equal to the maximum output of the device
a refractory period of 135 ms begins at the end of the charge; the first cycle following this refractory period is not counted (–)
the following 2 cycles are fast (VF), the shock diversion window has elapsed (500 ms after the end of charging); criterion 2/3 met.
41 Joule shock delivered on the second cycle (synchronized to the R wave)
the first atrial cycle following the post-shock refractory period (500 ms) is not counted (–)
the first ventricular cycle following the post-shock refractory period is not counted (–)
effective shock and termination of polymorphic ventricular arrhythmia
end of recording, although no end-of-episode marker is displayed
Take home message
this first trace illustrates the primary function of an implantable defibrillator: detection and treatment of ventricular fibrillation (an arrhythmia that is initially extremely rapid, polymorphic and disorganized) with a shock.
at the top of the first page of the PDF transmitted to the LATITUDE telemonitoring site you will find various pieces of information: patient’s surname, first name, date of birth , implantation center, remote monitoring center, device model and serial number, date of last face-to-face interrogation and date of last telemedicine transmission; the tracings in this book have all been anonymized; the ventricular tachy mode is set to «monitoring + treatment», which means that the full range of detection and treatment options is activated.
each recorded trace is numbered in chronological order (this is episode 42) along with the date and time of occurrence and information pertaining to the atrial and ventricular rate
the detail tab summarizes the main diagnostic and treatment steps undertaken for this episode; VF Event Onset: ventricular rate (321 beats/minute) and atrial rate (64 beats/minute) are calculated from the average of the 4 ventricular and atrial cycles preceding the V-Epsd marker; during V-Detect : atrial rate (65 beats/minute) and ventricular rate (297 beats/minute) are calculated by averaging the 4 cycles preceding the V-Detect marker; the episode is always detected in the VF zone; in this zone, no discrimination other than rate is used; on the other hand, various parameters are still recorded (stability, V>A frequency, Fib A, correlated Rhythm ID) even if they do not influence the decision to treat the episode; information on the various timers (SRD, ATP Time-ou t) is also displayed; Attempt 1, 41 J V Shock: the first therapy programmed in the VF zone is a 41 Joule shock; the duration of the charge was 9.8 seconds (expected for a maximum-output shock) with a lead impedance of 76 Ohms (expected for a single-coil lead); the shock waveform is biphasic and the nominal initial polarity corresponds to a cathodic shock (for a single-coil lead, the right ventricular coil is the cathode and the defibrillator can is the anode for the first phase, with polarities reversed for the second phase).
when a trace is analyzed from the programmer, it is possible to modify the scrolling speed (25 mm/s in the first instance); this can be useful for confirming the diagnosis of oversensing of a 50 Hz signal (scroll speed of 100 mm/s reveals a sinusoidal pattern with 20 ms between signals); calibration is adapted automatically by the device, but can also be modified from the programmer to facilitate manual measurement of the amplitude of the various signals
for each trace recorded on a dual- or triple-chamber defibrillator, 3 channels are nominally available: the bipolar atrial sensing channel (A), the bipolar ventricular sensing channel (V) and the shock channel (shock) between the distal coil and the can; the signal on the shock channel is similar to an electrocardiographic lead; ; markers and intervals are also available; compared with other manufacturers, Boston Scientific have chosen to provide a great deal of information on the trace, with numerous markers (for this example, atrial, right and left ventricular markers, PVARP prolongation , correlated cycles , etc.).)
to start recording an arrhythmia, 3 consecutive beats must occur in one of the tachycardia zones; the device then uses a sliding window during which it looks for the occurrence of 8 out of 10 consecutive rapid cycles; the first 3 cycles are included in this window; when this criterion is met, the V-Epsd marker appears on the trace; the duration starts from this marker; for Boston Scientific devices, a specified number of rapid cycles is not programmed for initial detection, but a duration during which the arrhythmia is sustained; an episode is considered sustained if a minimum proportion of 6 rapid cycles out of 10 is maintained throughout the duration; if, until the end of the duration, the 6/10 criterion is met, the device classifies the episode as VT, SVT or VF; when the duration ends, the last ventricular interval is analyzed to understand the dynamics of the arrhythmia: stable arrhythmia, slowing down or accelerating; if the last interval corresponds to the zone whose duration has just ended, therapies can be delivered; the end of an episode is declared after a duration during which the 8/10 redetection criterion is not met (10 seconds after untreated events, ATP treated events or after an aborted shock; 30 seconds after a delivered shock)
there are three programmable durations: initial duration (independently programmable in VF and VT zones), post-detection duration (when a charge has been diverted or after an ATP sequence; programmable in the VT zone, fixed at 1 second in the VF zone) and post-shock duration (after a shock has been delivered; programmable in VT zone, fixed at 1 second in VF zone)
the interval plot provides an overall view of the episode, with a number of characteristic aspects to be aware of (railroad track appearance cases of P wave oversensing , T wave oversensing or double counting of the R wave, cloud of points with very short cycles in the case of lead dysfunction, undersensing with long cycles in the case of a VF episode, etc.).); interval plot analysis is therefore an integral part of reading the various tracings, and should probably be the first step before detailed analysis of the EGM.
This figure shows the 3 available channels with a good-quality color EGM plot and a multitude of markers (lots of information, the plot is sometimes a little busy).