Counting in the VT zone
Patient
A 61-year-old male was implanted with a dual-chamber device for dilated coronary heart disease with compensated heart failure and an ejection fraction between 30 and 35%. The
patient consults for a systematic follow-up control.
Overview screen
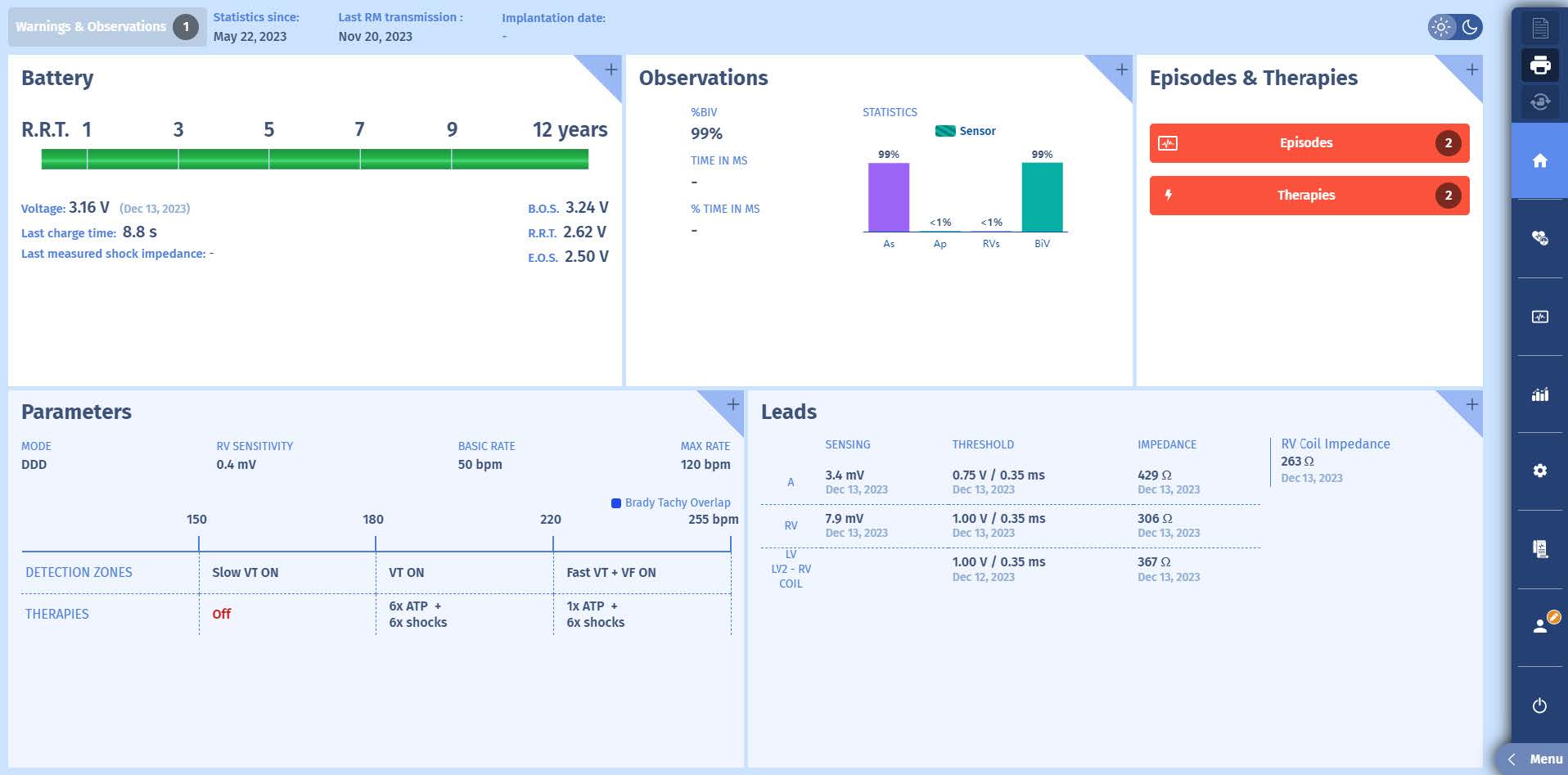
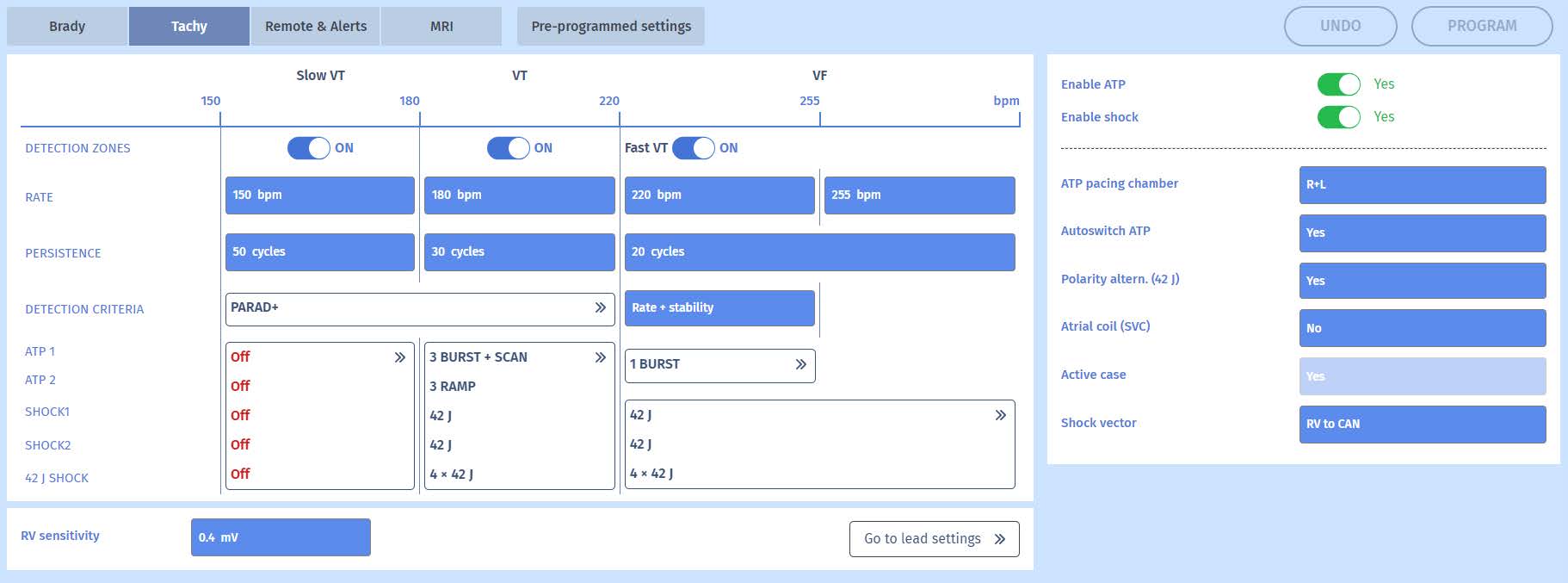
Programming
 Episode (first screen)
Episode (first screen)
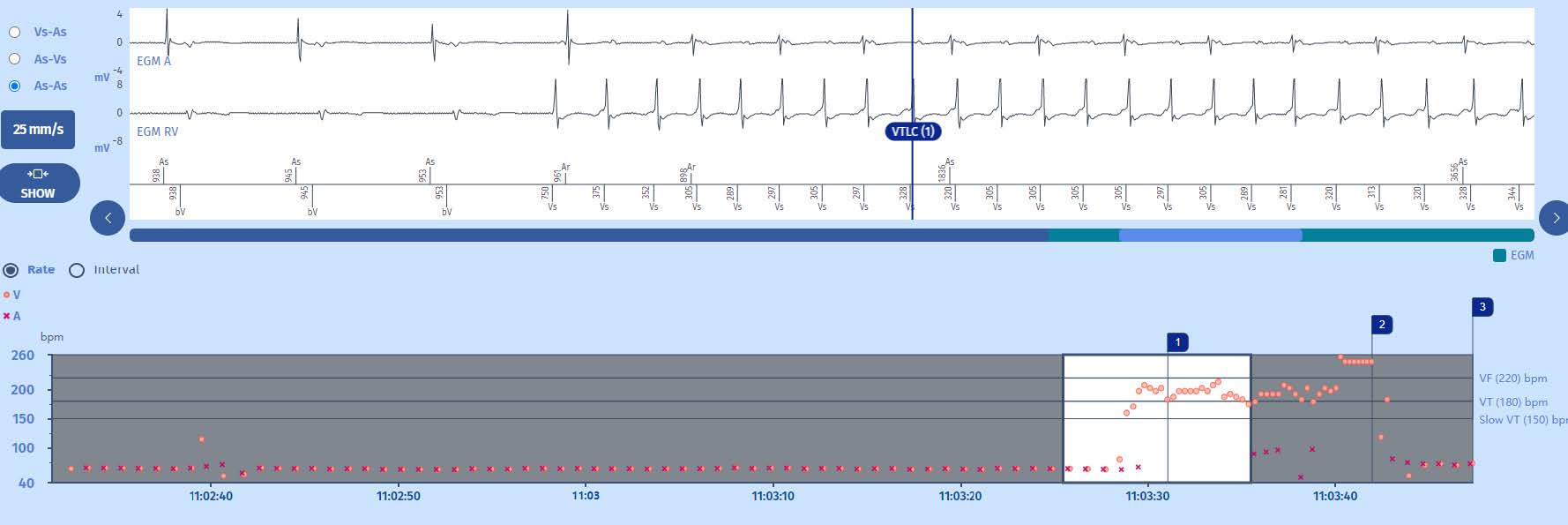
Overview of the full EGM
Tracings: The tracing at the top is the atrial electrogram, underneath, the ventricular electrogram, and lastly, at the bottom, the atrial markers above the line and ventricular markers below, along with the time intervals.
Trace
The tachogram
1 The rhythm is sinus with biventricular resynchronization.
2 Ventricular tachycardia begins in the VT zone (orange dots), while the atrial rate remains slow (purple crosses (x)).
3 An ATP is delivered with a return to sinus rhythm in the Slow zone.
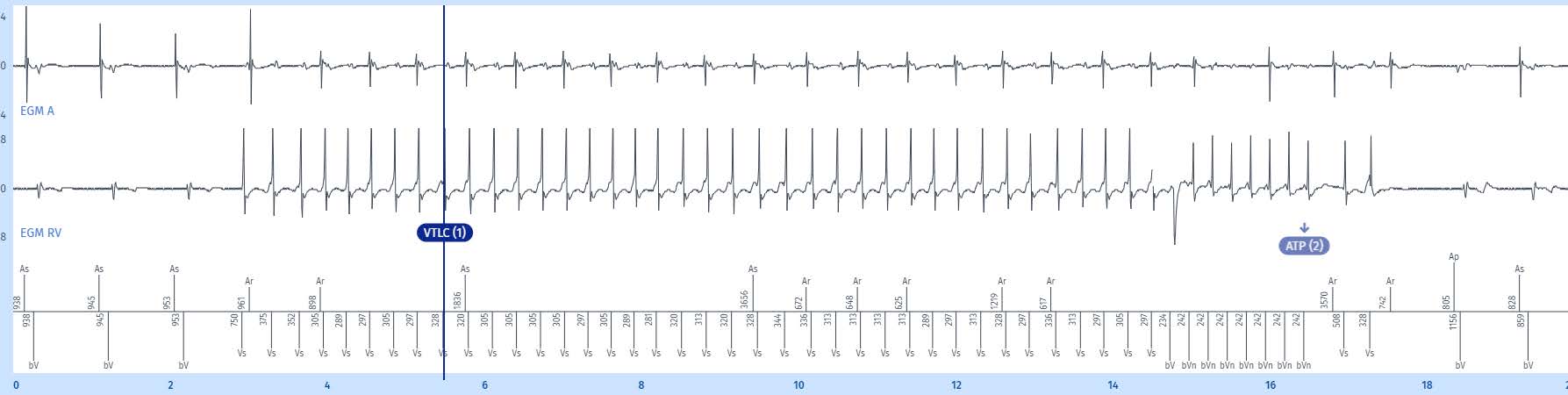
EGM
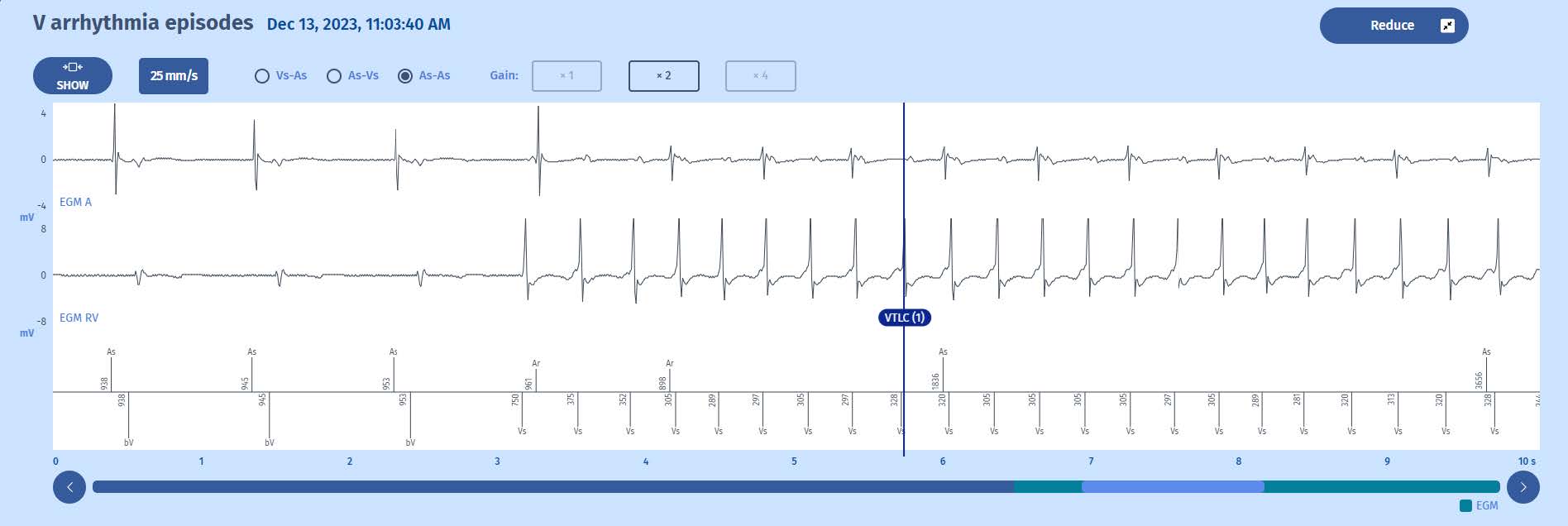
1 The rhythm is sinus with synchronized biventricular pacing
2 Ventricular tachycardia begins. The first tachycardia cycle (750 ms) is outside the tachycardia zone (400 ms). For the defibrillator, the tachycardia begins at the next cycles which are in the VT zone ((375 ms, 352 ms < 400 ms). In the VT zone, the first 2cycles are axcluded. The next 6 cycles are all in the VT zone and count towards the majority. The rate is on average 200 / min zo well within the VT zone (>180/min). The 6 out of 8 cycles in the VT zone criterion is fulfilled. The ventricular rythm is stable and there is an atrio-ventricular dissociation (more ventricular than atrial signals). The marker is: 1 (VTLC). The persistence phase begins.
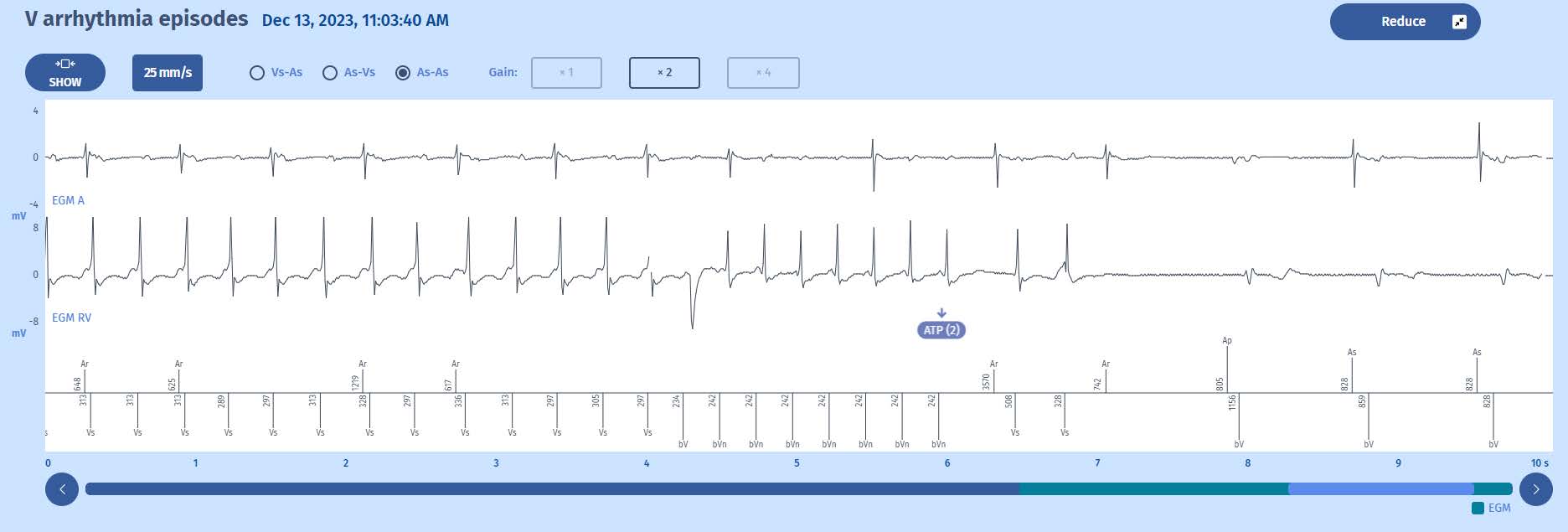
3 After 30 persistence cycles during which all cycles are in the VT zone, an anti-tachycardia pacing burst is initiated for 8 fixed cycles (this is the first therapy programmed in this
zone), shown by the second marker: ATP (2).
4 The ATP is effective with termination of the tachycardia, and after 6 slow cycles (and a PVC at 328 ms), the episode is terminated (label: Slow Rhythm).
Comments
1 This episode shows the perfect detection of a ventricular tachycardia. The counting is carried out according to the 6 of 8 cycles rule: 75% of cycles in a programmed VT
zone triggers a persistence phase that is programmable in cycles (in this instance 30) during which the cycles must validate a majority rhythm (6 out of 8 cycles) in a VT
zone and are analysed for diagnosis. If a Slow cycle (excluding VT zones) is detected, it does not reset the persistence counting to zero. The VT persistence counting is
set to zero if a majority of Slow cycles is detected or a majority of SVT/ST rhythm. In addition, there is no distinction between VT and Slow VT during the counting of VT
persistence: it is only at the end of the VT persistence (the shortest) that the devicecalculates the averaged rate of the last 4 cycles to determine if the rhythm is in the
VT zone or in the Slow VT zone. In the present example, all of the cycles are in the VTzone. If the cycles enter in VF, the diagnosis of VF is made if the majority rate (6/8)
is VF.
2 The averaged rate of the last 4 cycles in the Tachy/VF zone calculated at the time of persistence determines the type of therapy that will be initiated after the
persistence phase. The first therapy programmed in the VT zone of our patient is therefore launched (an 8-cycle burst with a pacing interval equal to 80% of the
average coupling interval of the tachycardia). In this case the average RR intervalwas 305 ms (197/min) resulting in an ATP of 242 ms (248/min).
3 Note: not all atrial events are sensed given that, due to atrio-ventricular dissociation, some fall into the post-ventricular atrial blanking period; during the ATP, the ventriculograms are only captured completely starting at the 2nd cycle of the burst.
4 The therapy was effective, and thus the programming will not be changed.
Take home message
1 The counting follows the rules of the majority rhythm. At least 6 out of 8 cycles must be in a programmed zone for an initial diagnosis to be made.
2 The persistence phase must be completed to establish a final diagnosis and is recommended at 30 cycles.
3 In the VT or Slow VT zone, the last 4 persistence cycles determine the type of therapy of the tachycardia zone that will be applied.

