

A 70-year old patient is implanted with a dual lead ICD (ULYS DF4) in the context of secondary prevention (VF) in ischemic cardiomyopathy. You interrogate the device in the emergency department after sensation of a shock.

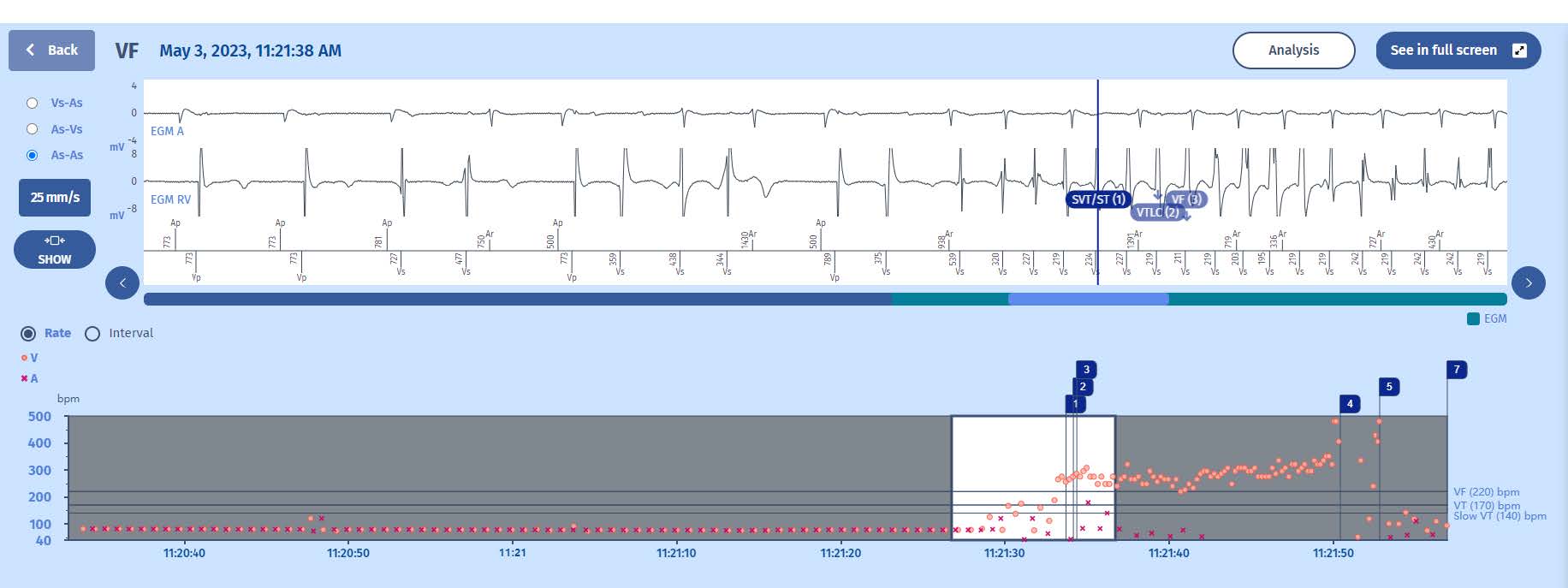

The interval plot shows a stable atrial and ventricular rhythm (probably paced as the intervalsseem fixed) with a sudden acceleration of ventricular events, beginning with extrasystoles and continuing with a more organized tachycardia in the VF zone. After the shock (marker 4), there are again a few extrasystoles before the return to slow rhythm).
EGM
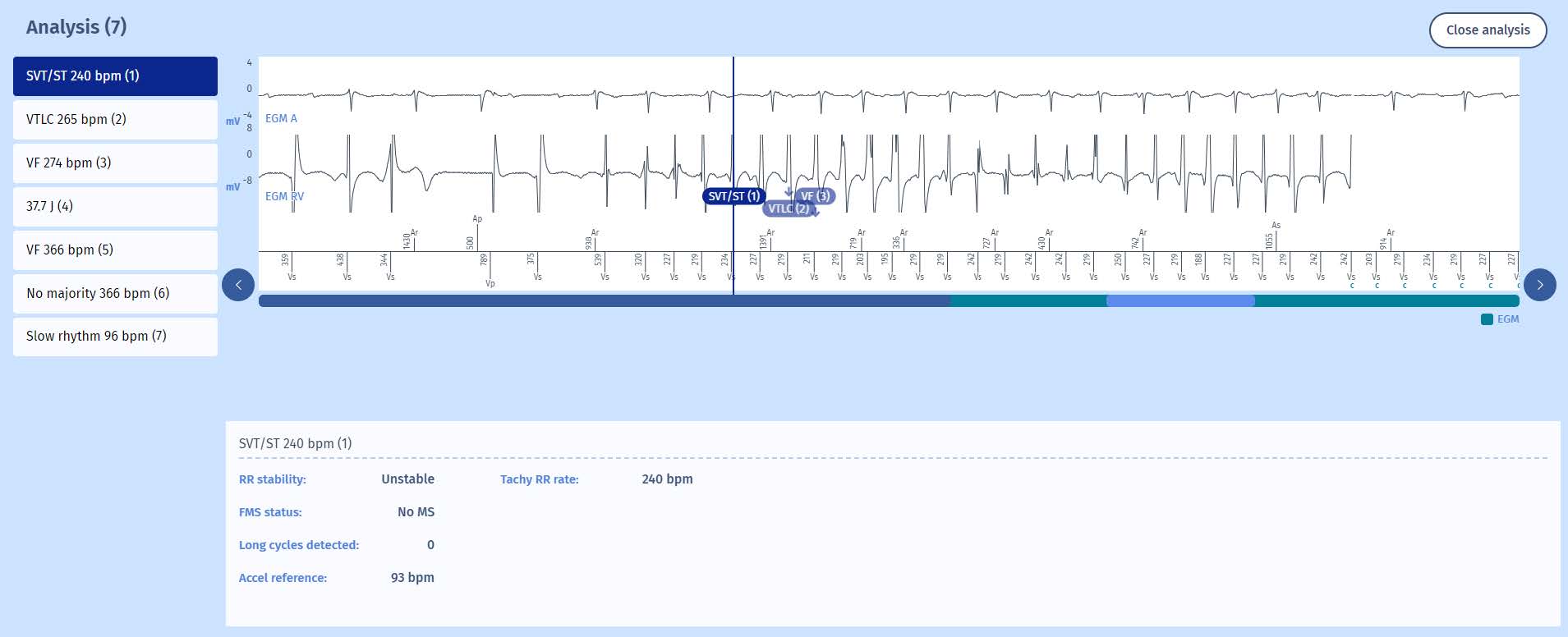
The beginning of the tachycardia is very typical with first extrasystoles disturbing the rhythm and then an organized ventricular arrhythmia which speeds up and becomes more organized after a few cycles. This is called “warming-up” and is often seen in the beginning stage of a fast ventricular tachycardia. As MicroPort ICDs use a very fast counter (6 out of 8), we often see an early SVT marker during this period as there are 6 cycles in the VT zone (including 2 extrasystoles) but these cycles are unstable and therefore the discrimination algorithm classifies the events as “supraventricular”(SVT). When we click on the marker, in the window we find the word: Unstable, which confirms the normal algorithm behavior.
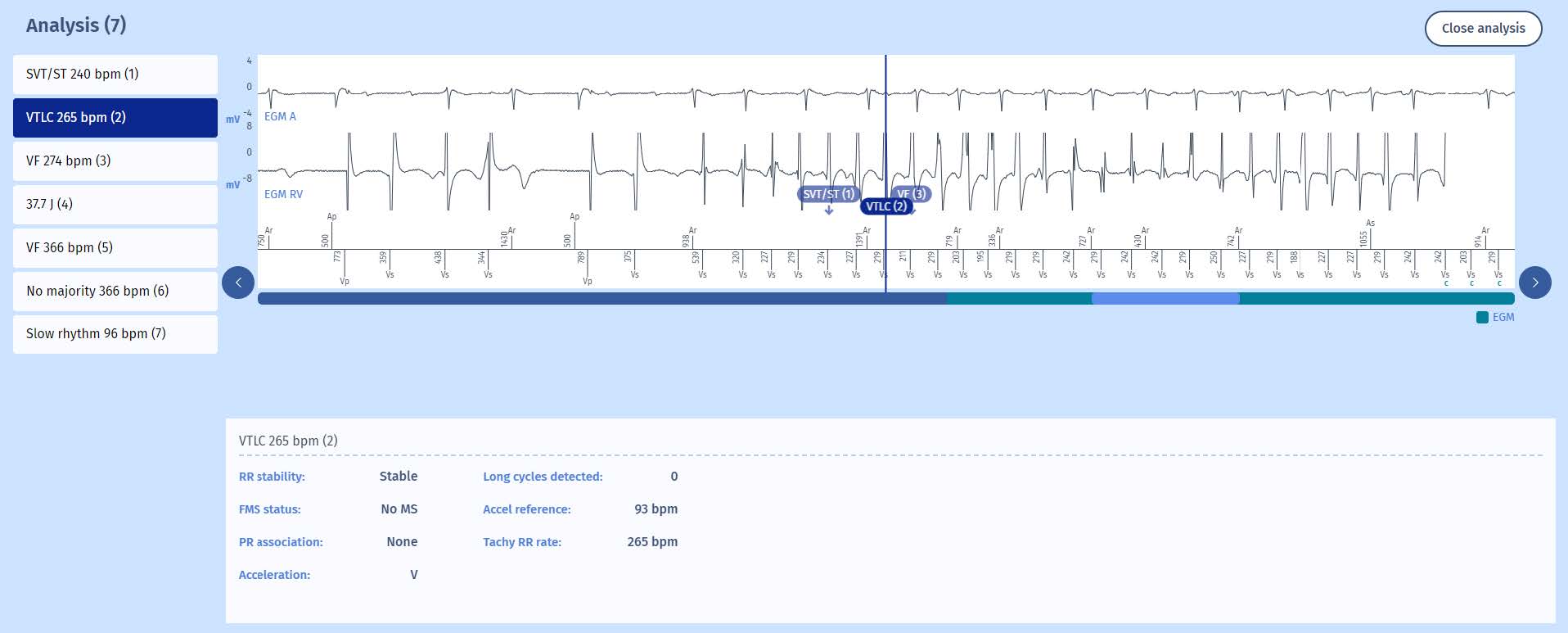
As the arrhythmia speeds up into the VF zone, there is fast appearance of the VF marker and theVF persistence starts (at a value of 1) while the VT persistence increases to 2 (it was 1 during the previous cycle at the same time as the VTLC marker). There is no discrimination in the VF zone in MicroPort ICDs so any 6/8 events in the VF zone will result in a VF marker. There is however another check of stability which is required to make the choice between Fast-VT or FV therapies but more about this later. After filling of the VF persistence (20 cycles), the charge begins.
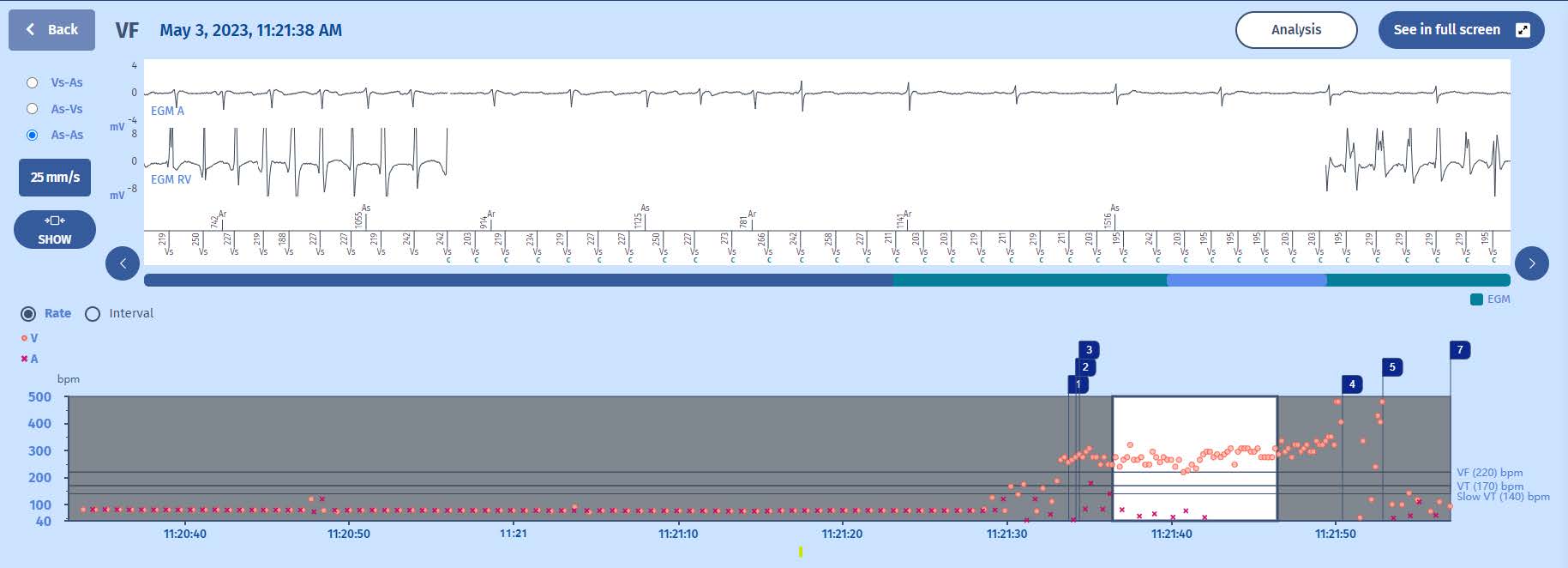
After the charge has completed, there is confirmation of the tachycardia and the shock is delivered. The shock terminates the VT. Interestingly, there is a new VF marker which is caused by some low amplitude noise on the ventricular channel, associated with some late post-shock artifacts. But the persistence is reset soon after when the VF majority is lost (No majority marker). The episode is concluded when the Slow majority is reached.
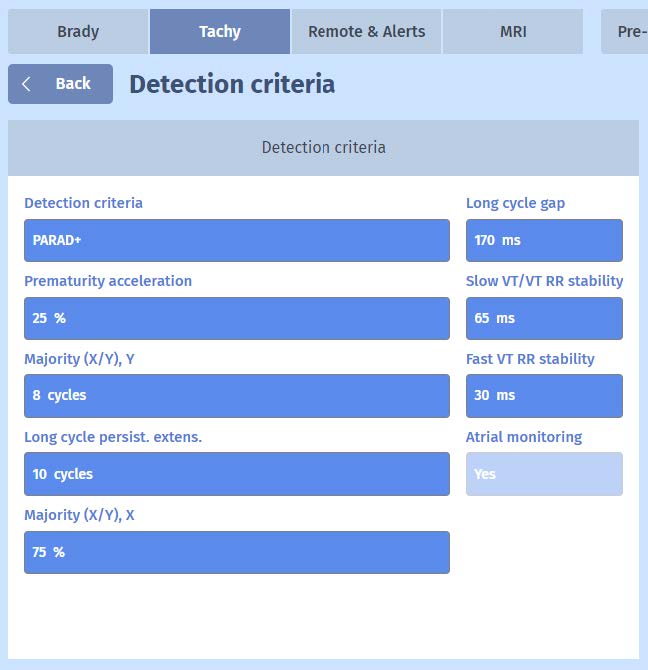 Under “Tachy” parameters, we can find
Under “Tachy” parameters, we can find
and modify the X out of Y Majority. By
defaut, Majority is set to 75% (X) out of 8
cycles (Y) and these parameters should
not be changed.