A 72-year-old man with a triple-chamber defibrillator for dilated heart disease with healthy coronary arteries, an ejection fraction of 28%, complete left bundle branch block, and optimal medical therapy. The patient has never experienced a VT until now, and is
known with paroxysmal AF. The patient consults due to a loss of consciousness the day before.
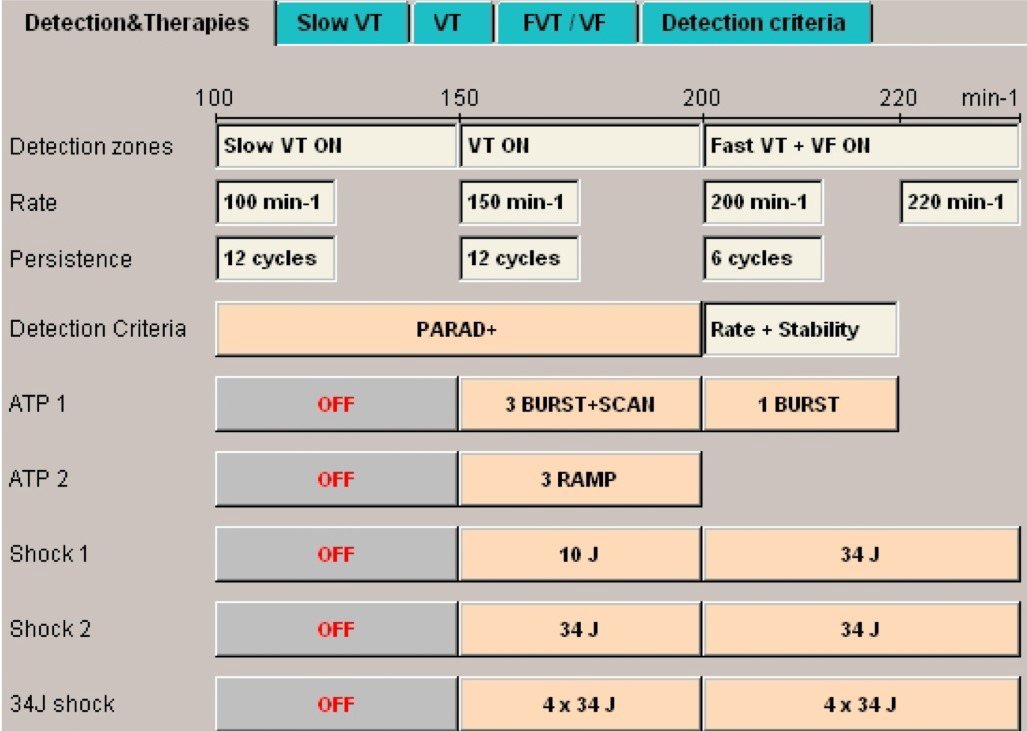
Programming
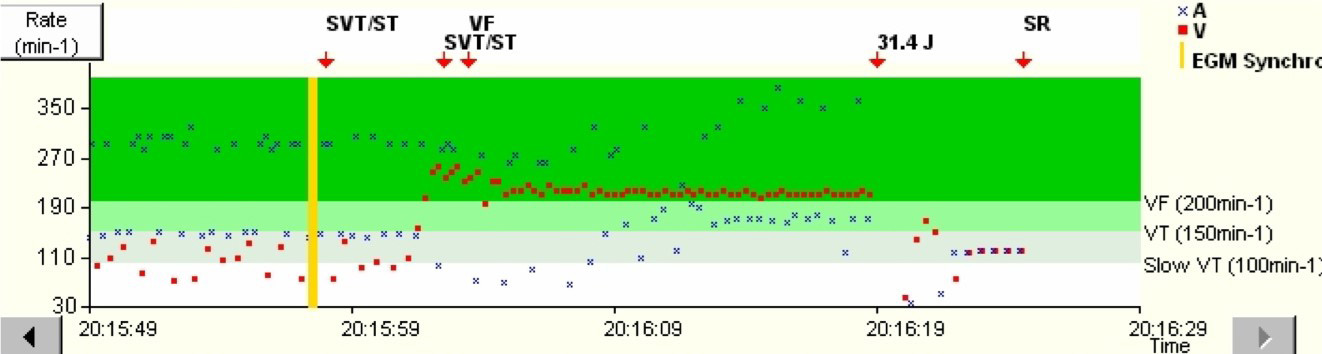
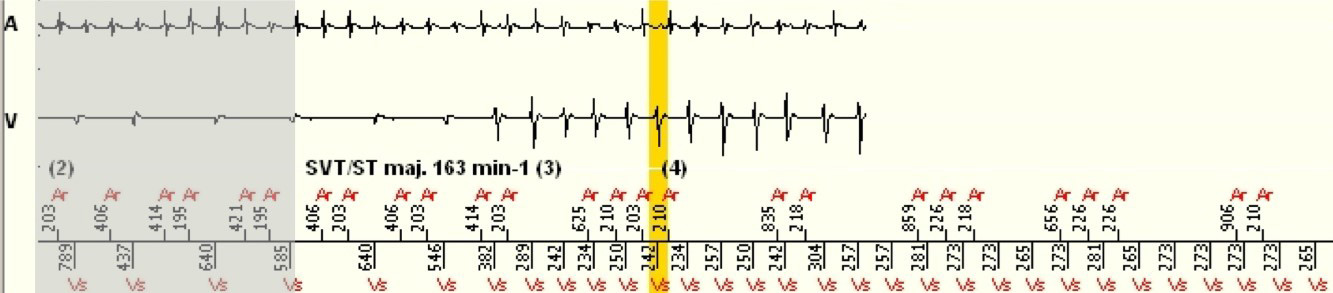
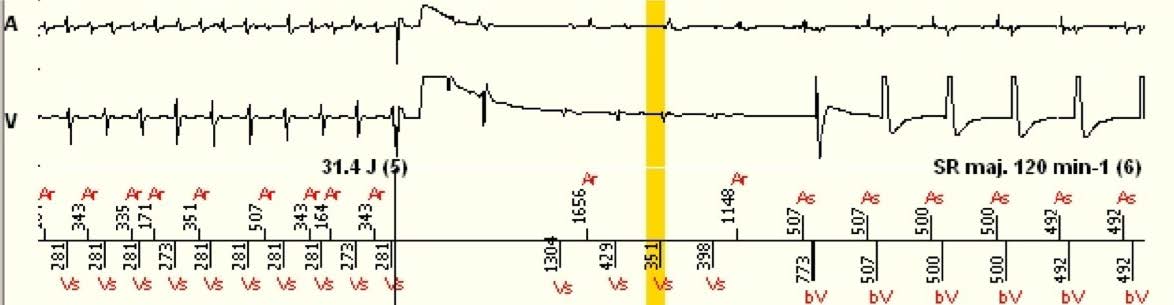
Interval plot
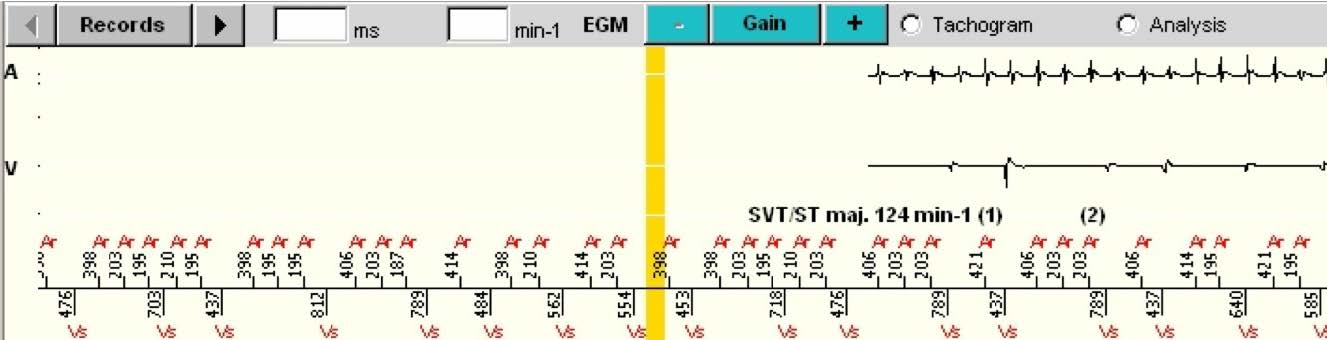
The shaded areas are the portions of the EGM that are the repetitions of the end of the previous image.
Interpretation