

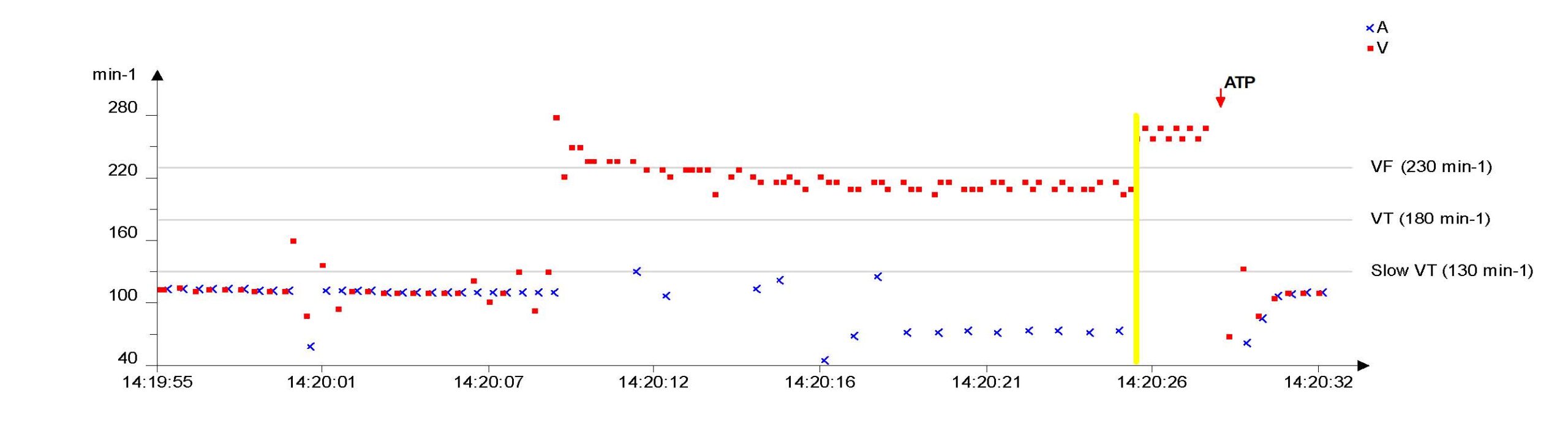
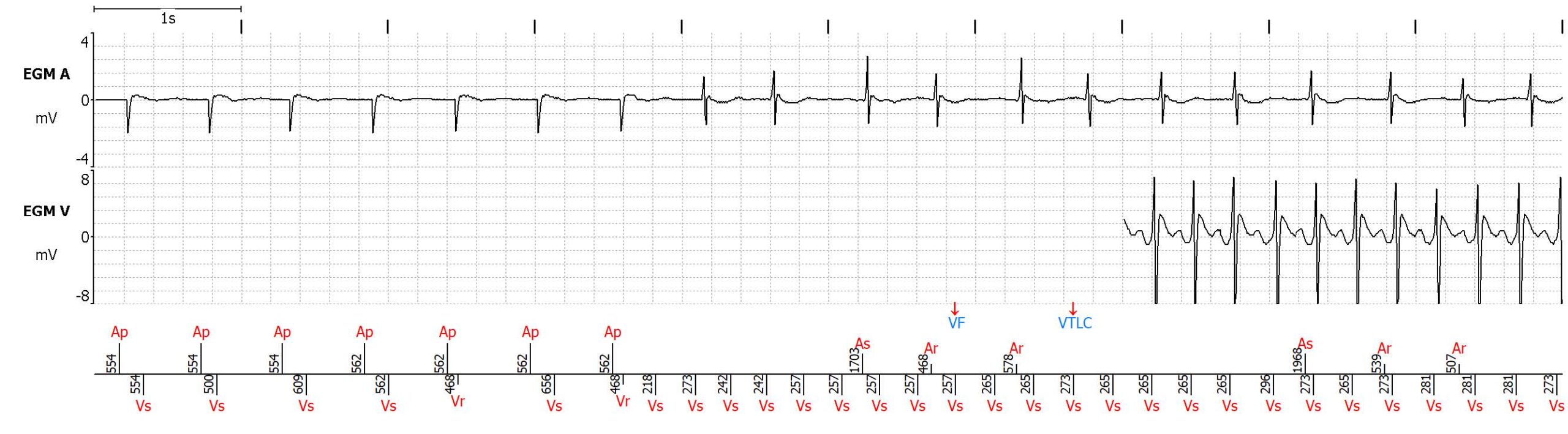
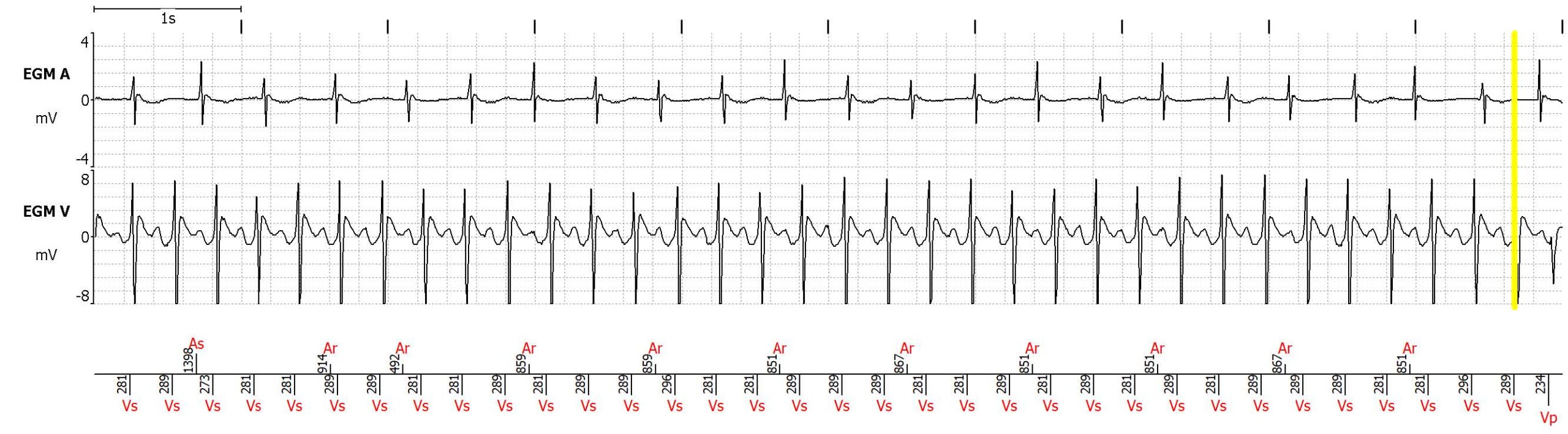
The transmission includes an episode showing a ventricular tachycardia at around 210 beats per minute. The sensing of ventricular events is correct and there are no signs of noise artifacts.
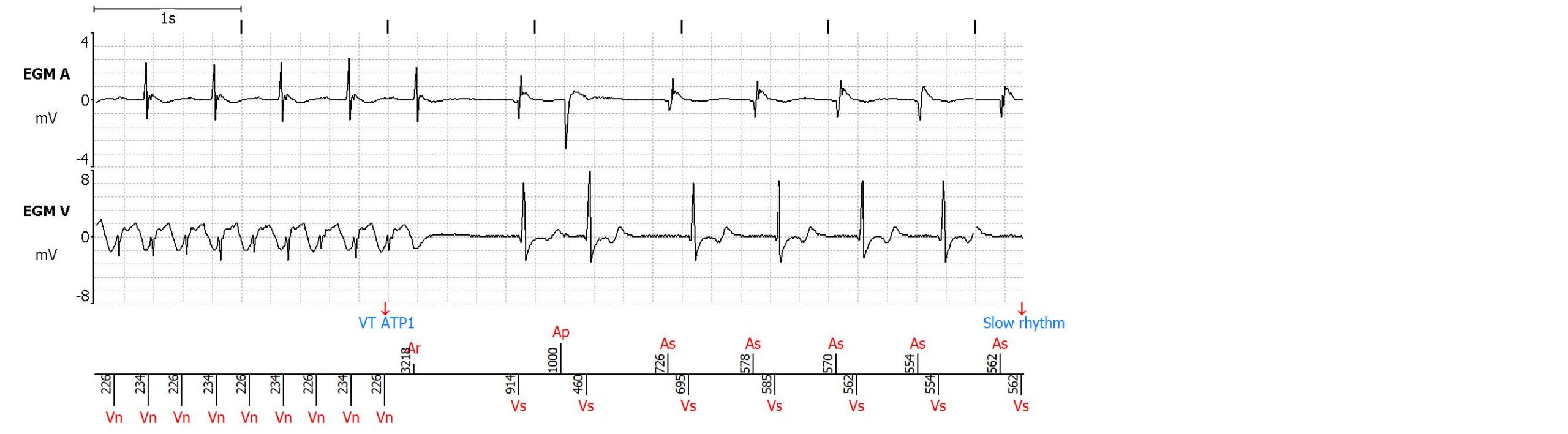
After a few cycles in the VF zone, the VT stabilizes in the VT zone with correct classification (VTLC marker). However, it takes over ten seconds for the VT to be treated, as the persistence counter is programmed to 50 cycles, instead of the recommended 20 or 30 cycles. Then the ATP terminates the VT with success.
Next steps
Treated ventricular arrhythmias often need clinical action. After making sure the ICD and leads function properly, the clinical history of the patient should be collected to be able to understand
why programming is different from the recommendations. In this case, it is because this young patient (50 years of age) implanted due to a dilated cardiomyopathy is known to have asymptomatic nonsustained VTs, even at high rates. It was previously decided to program longer persistence counters, in order to allow for the VT to self-terminate, and decrease the risk of deleterious ATPs (bursts or ramps which accelerate the VT into faster VT or VF). It is however recommended to call the patient to enquire whether the episode was symptomatic (especially if loss of consciousness occurred) which may require reprogramming the ICD. The persistence counter is a compromise between the willingness to treat ventricular arrhythmia
before it causes symptoms or accelerates into a more dangerous arrhythmia, and the willingness to reduce unnecessary therapys. It is important to note that successful ATP/shock does not mean that is was needed, as many ventricular arrhythmias self-terminate. This is a limitation of many (older) ICD studies. The ideal persistence is probably not to be defined for all patients, but rather at patient