- ATP Quick Convert is the anti-tachycardia pacing sequence that can be delivered in the VF zone of a Boston Scientific defibrillator; it is ATP before charge.
- ATP before charging reduces energy consumption; once VF has been diagnosed, ATP is delivered; if VF is reconfirmed after ATP has occurred, capacitor charging begins; if arrhythmia terminates, charging is not initiated; this saves capacitor charging if ATP is effective; on the other hand, if ATP is ineffective, it delays shock delivery by 2 to 3 seconds
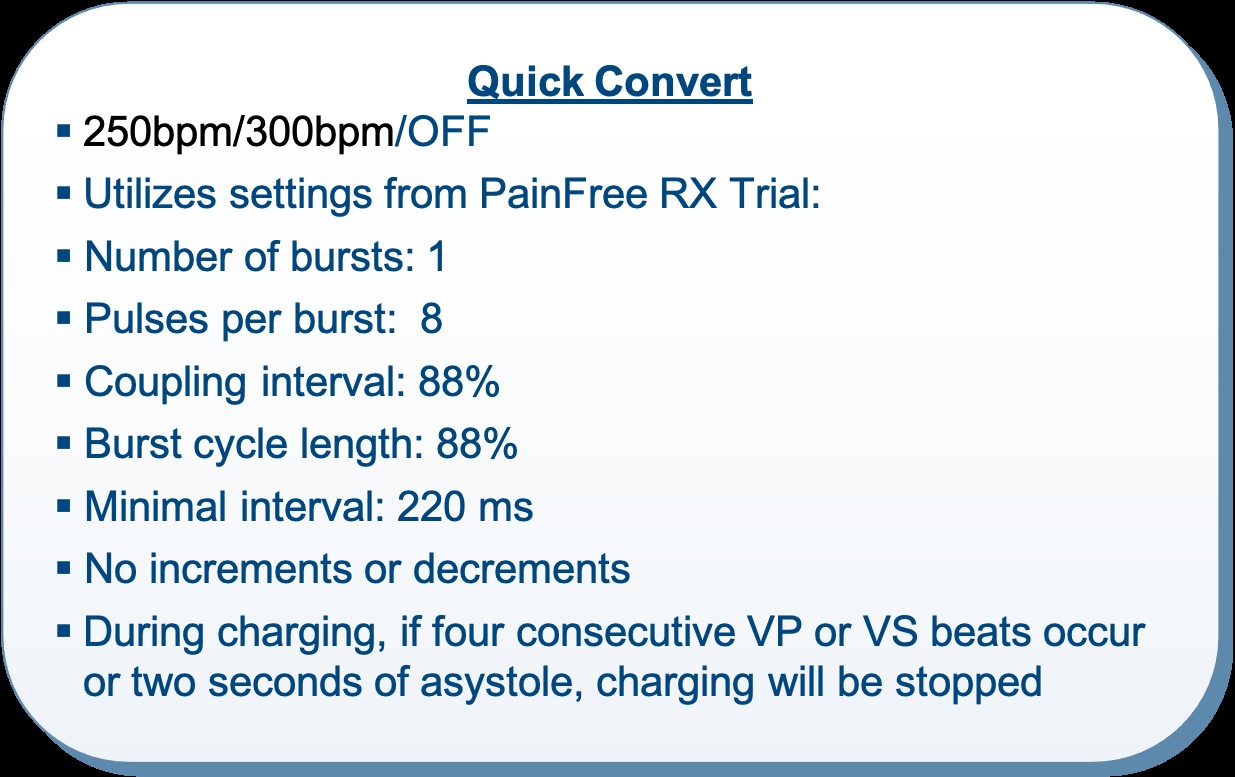
- this pacing sequence can only be delivered following initial detection in the VF zone, if the tachycardia sequence does not exceed 250 or 300 beats/minute (programmable on the latest platforms).
- the characteristics of this anti-tachycardia pacing sequence are not programmable: it is a burst of 8 stimuli with an 88% coupling interval
- following this sequence, the device evaluates the effectiveness of the therapy; if at least 2 out of 3 cycles are considered slow, charging is cancelled; conversely, if at least 2 out of 3 cycles are considered fast, charging of the capacitors begins.
- in this example, ATP is not only ineffective but also accelerates tachycardia; a real-life study carried out on Boston Scientific defibrillators showed that, while the effectiveness of a first-line shock for an episode of VF averaged 90%, this success rate fell when the shock was delivered after an anti-tachycardia pacing sequence; one explanation lies in the risk of acceleration, as in this example, from a monomorphic arrhythmia to a very rapid polymorphic arrhythmia, with an increased risk of an ineffective shock; if ineffectiveness or a pro-arrhythmic effect is observed, it is advisable to deprogram the anti-tachycardia pacing sequence
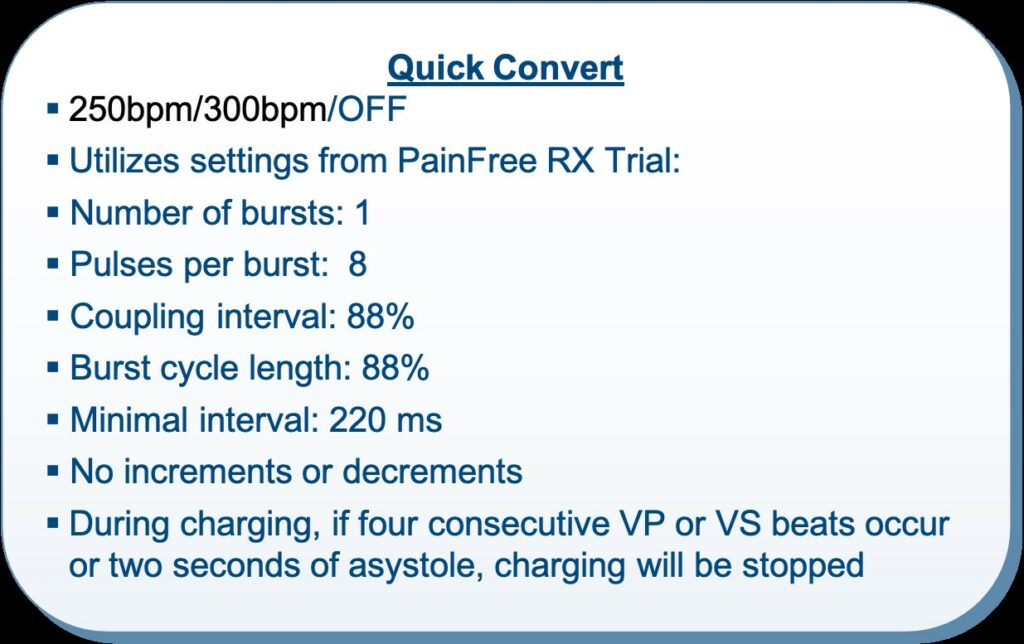
Characteristics of anti-tachycardia pacing in the VF zone: the tachycardia frequency limit up to which ATP will be applied is programmable at either 250 or 300 beats/minute; other parameters are not modifiable (1 burst, 88% coupling, 8 stimuli).