

Once the burst has been delivered, the device analyzes the rhythm: if the arrhythmia persists, charging of the capacitors begins; if the arrhythmia has stopped, charging does not begin.
The device uses the following criteria to assess burst efficacy:
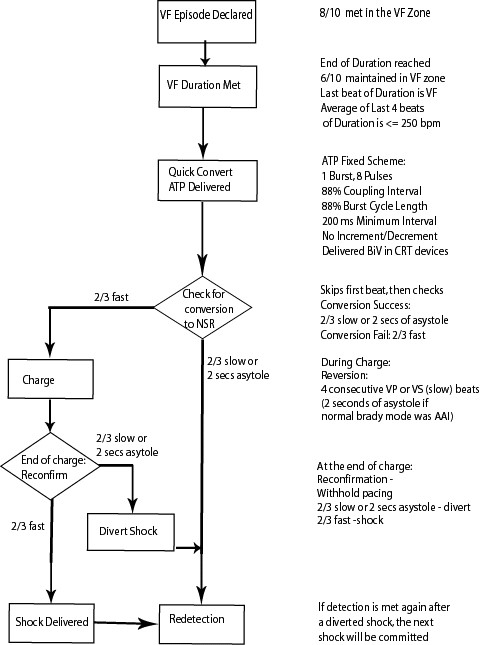
This figure shows how the Quick Convert algorithm works (anti-tachycardia pacing in the VF zone).