Appropriate discrimination? Analyse everything!
Patient
A 65-year-old man implanted with an INTENSIA DR dual-chamber defibrillator in secondary prevention for post-infarction dilated ischemic heart disease with highly altered ejection fraction, stage III heart failure and narrow QRS.
Programming
3 zones with:
- A Slow zone starting at 125/min, 30 persistence cycles, with ATP and shock sequences
- A VT zone starting at 185/min
- A VF zone starting at 240/min
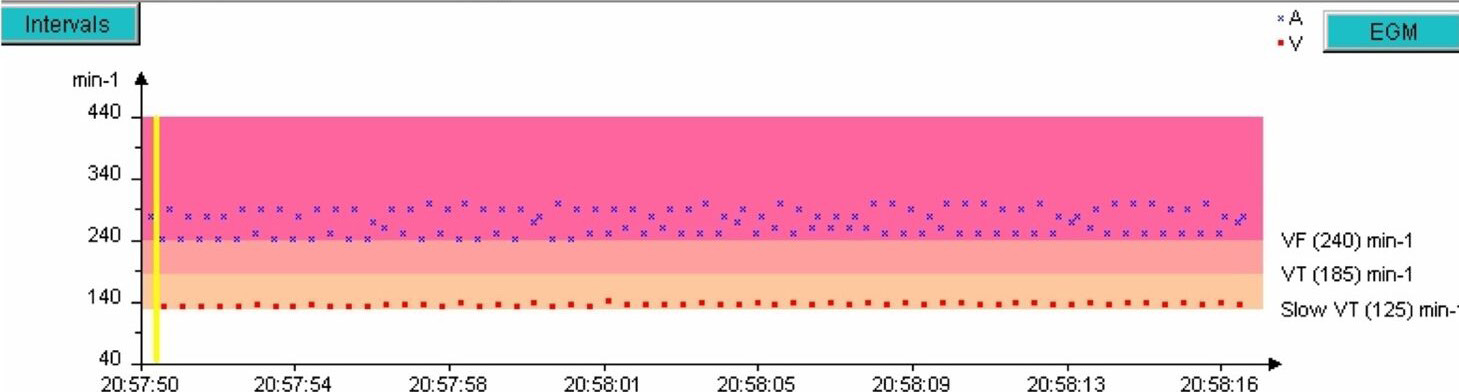
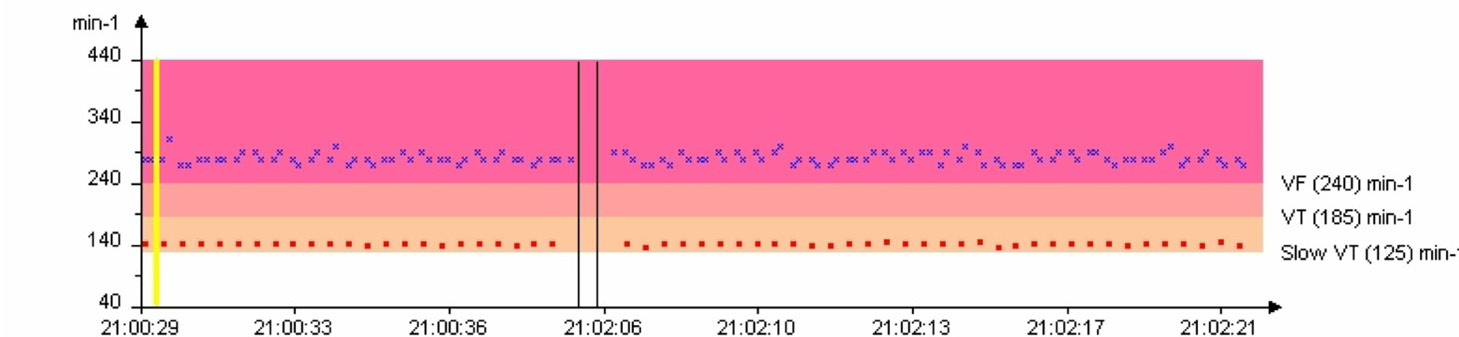
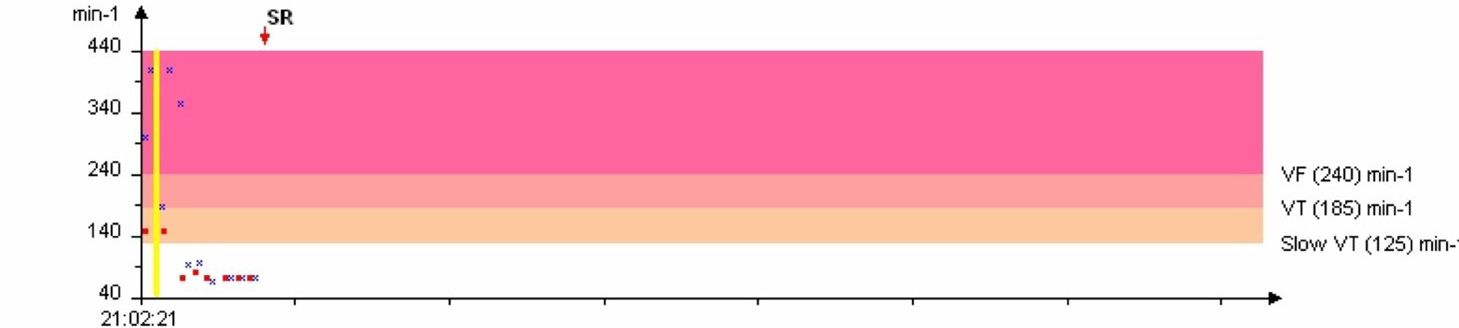
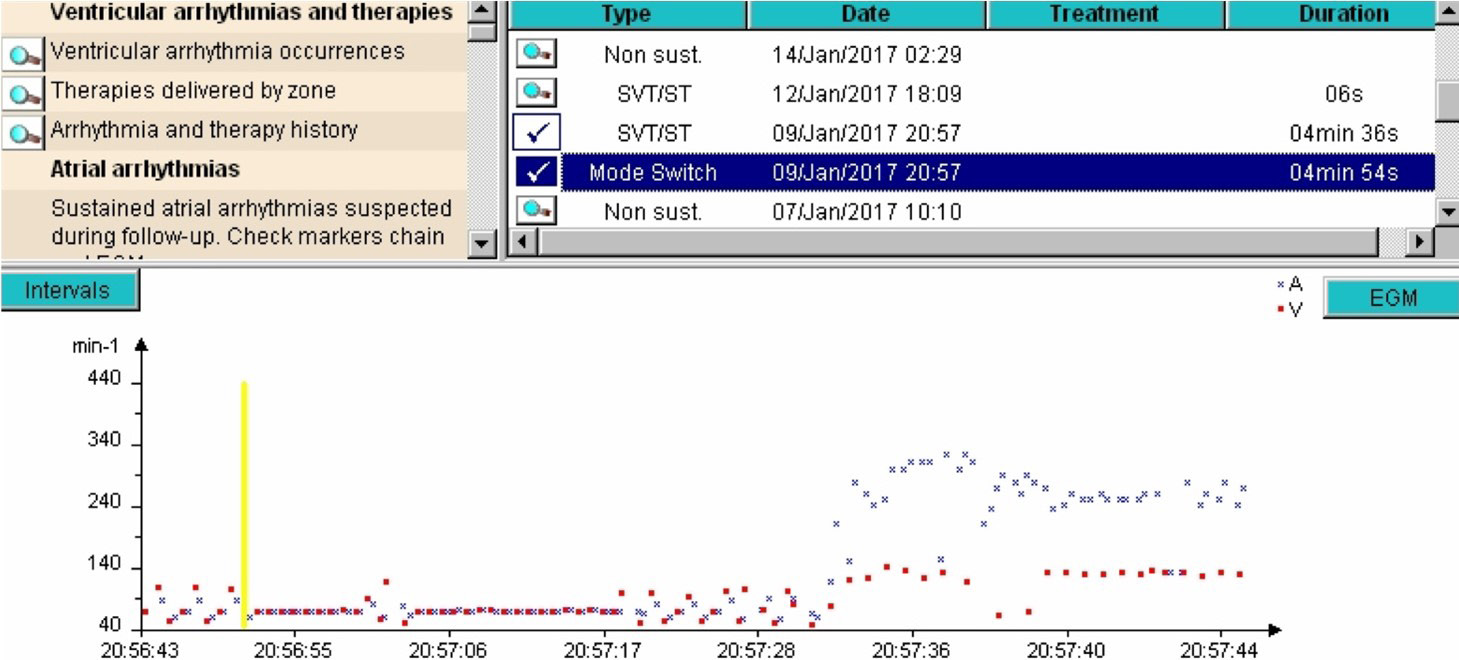
Rate interval plot
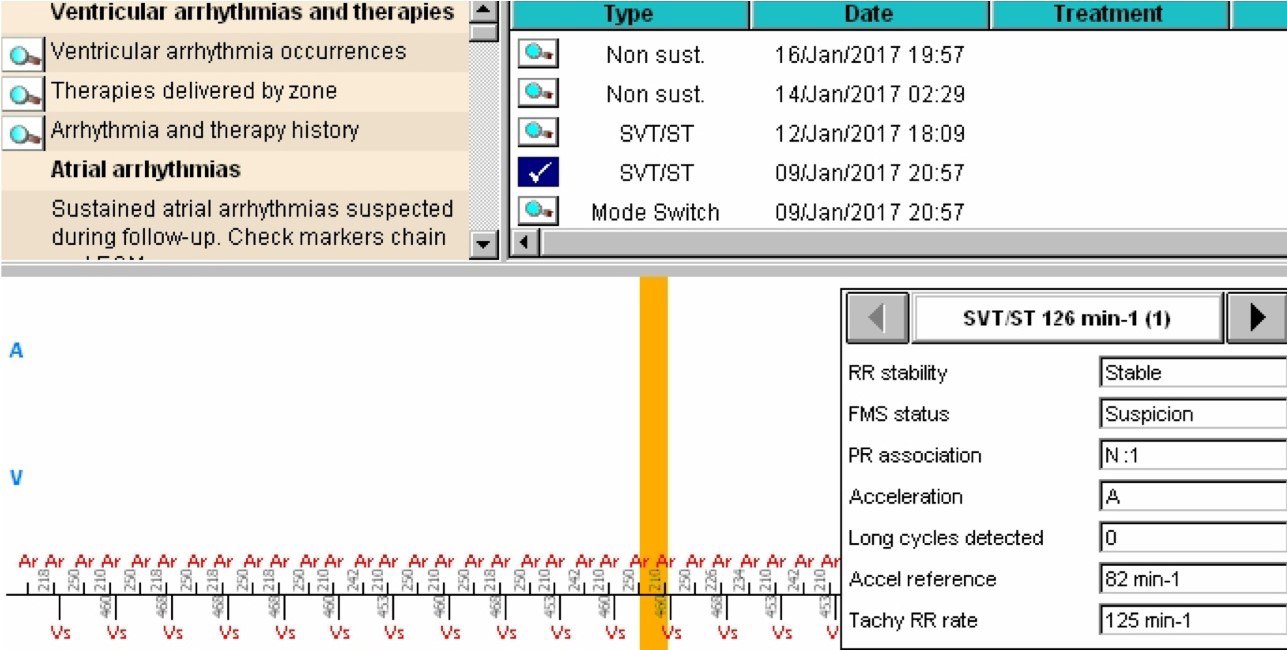
EGM
Interpretation
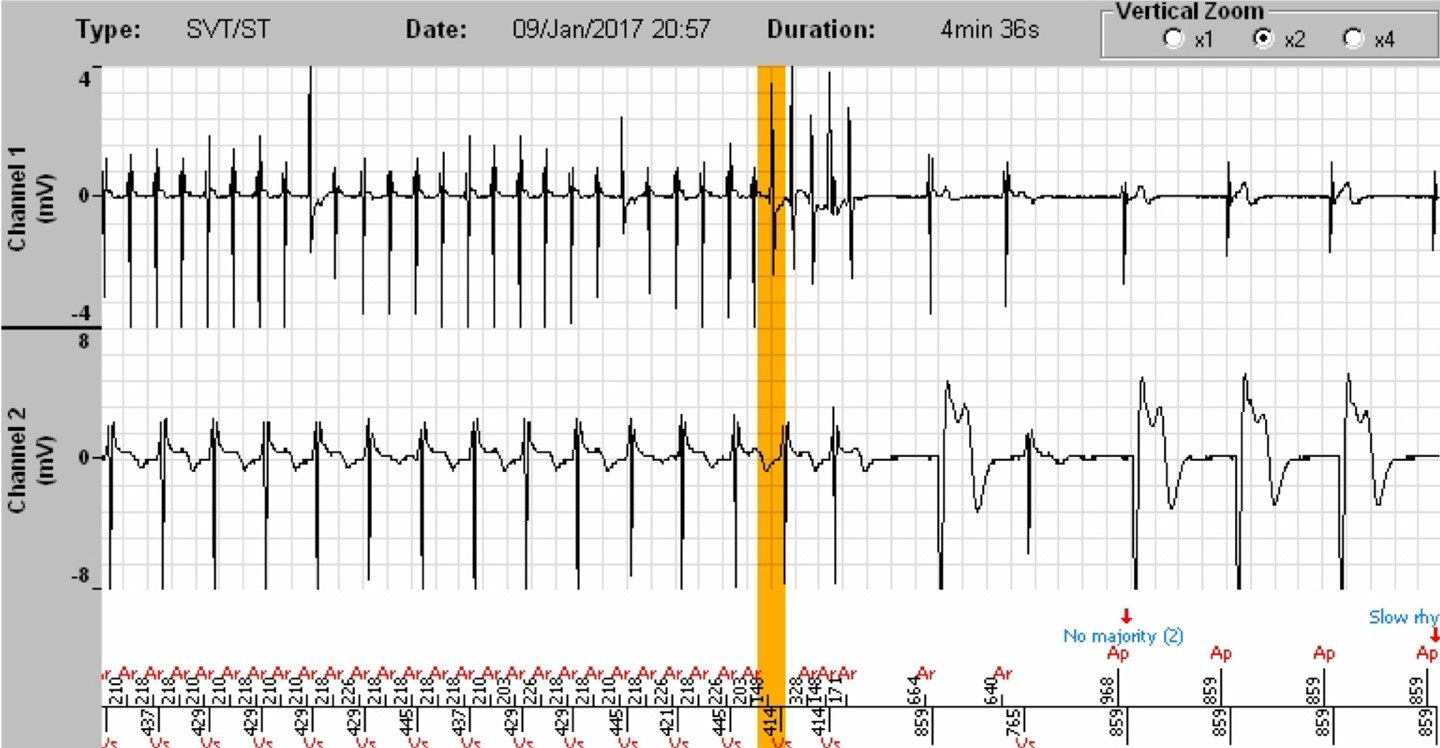
- The defibrillator documents a SVT episode in the list of stored episodes, whose duration was 4 minutes 36 seconds. The start time of the tachogram is 20:57:50. The onset of the tachycardia is not visible. The termination of the tachycardia can be analysed with a Slow Rhythm majority return that marks the end of the episode.
- The defibrillator documents a stable tachycardia with an N:1 (2:1) PR association, a sudden onset by way of an atrium, and is in mode switch (state of suspicion). The criteria that led to the diagnosis of SVT are therefore stability and N:1 PR association.
- In fact, by looking more closely at the list of stored episodes it is found that on the same day, and at the same time, a mode switch is reported which lasted 4 minutes and 54 seconds and thus covers the SVT episode reported at the same time. The beginning of the tachycardia is therefore analysable, but within the mode switch episode. Impractical, given the functioning principles of the Fallback Mode Switch and PARAD+ algorithms as well as the management of stored data. To summarise, the Fallback Mode Switch will identify an atrial arrhythmia after 28 ventricular cycles involving PACs while PARAD+ will recognise this same arrhythmia after 38 ventricular cycles (2 initial cycles not taken into account, 6 for the first majority and 30 for the persistence) with the criteria of SVT fulfilled. Moreover, the EGMs and markers are not “duplicable”, i.e. once the EGM/markers corresponding to the fallback mode switch criterion are memorised/stored, they are no longer usable for the next episode (in this instance, the SVT identified by PARAD+).
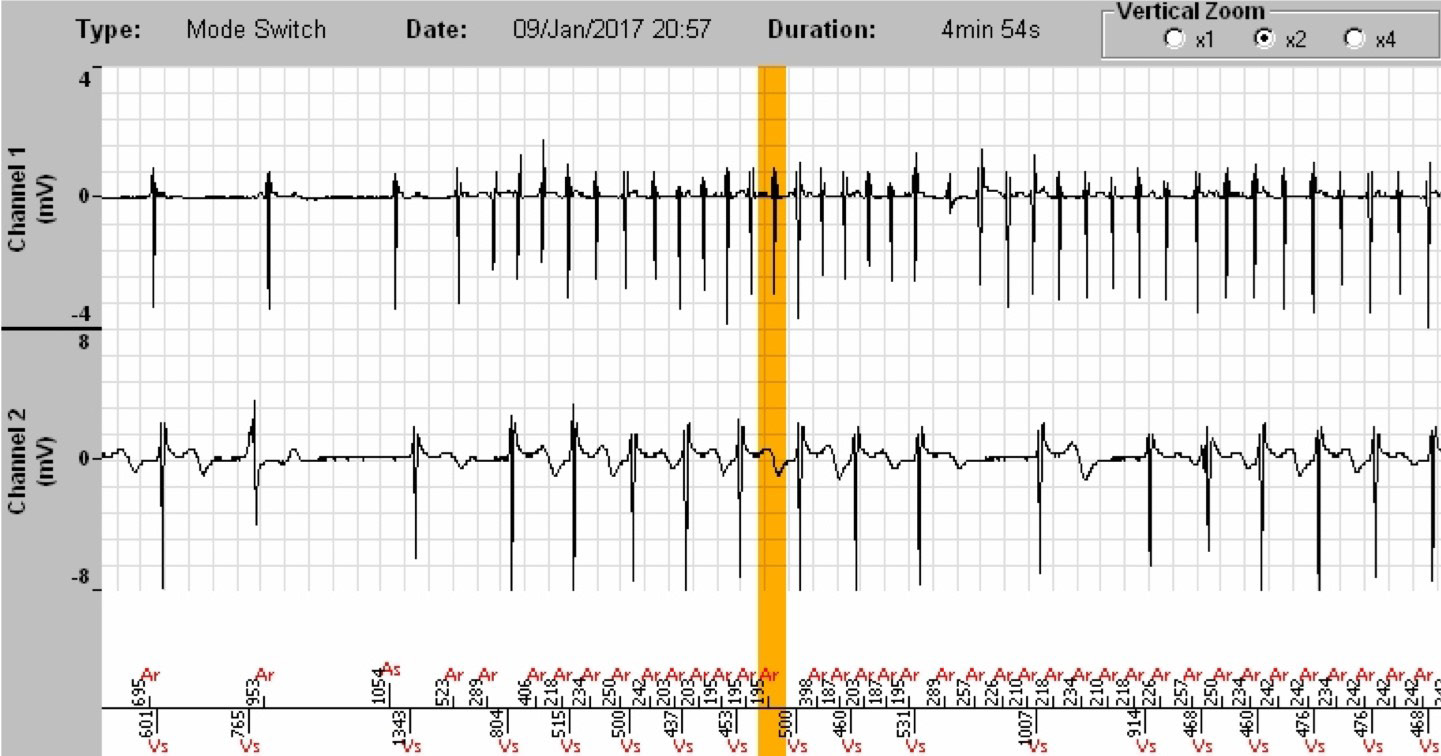
- In this instance, we can declare that the tachycardia is supraventricular. Following a phase of sinus rhythm instability linked to PVCs, the atrial tachycardia begins with variable AV conduction at 20:57:30, which causes the defibrillator to enter into suspicion of mode switch and then to actual mode switch. The ventricular rhythm becomes stable approximately 10 seconds after the onset. The continuation of the mode switch episode constitutes the episode labelled SVT.
Comments
- The diagnosis was appropriate since the algorithm perfectly identified the onset of the tachycardia as being stable with N atrial events for 1 ventricular event (2:1 specifically). This is the essential element that allowed the diagnosis of SVT.
- The diagnosis of SVT was maintained until the spontaneous termination of the atrial arrhythmia.
- However, for the observer, it is necessary to retrieve the information in two different stored episodes: one pertaining to the pacing component of the defibrillator, the other pertaining to the discrimination algorithm of the defibrillator, which renders the
reading quite difficult.
- The placement of the atrial lead of the MicroPort dual- and triple-chamber defibrillators requires meticulous care in order to limit as much as possible detection defects of the arrhythmic atrial signals which the algorithm needs for an effective discrimination.
In the absence of visualisation of the onset of a tachycardia episode, it is necessary to look for this onset in another stored episode of the memorised list. This mainly concerns atrialarrhythmias, as in the present example, with the beginning of the arrhythmia most often found in the mode switch episodes since the Fallback Mode Switch algorithm is faster in classifying this type of arrhythmia than the PARAD+ discrimination algorithm, programmed with a persistence of more than 20 cycles. In other words, this happens when the device goes into switch mode before the end of the PARAD+ algorithm persistence.

