72-year-old male implanted with a Momentum triple-chamber defibrillator
Summary
episode initially classified in the VT zone then in the VF zone
1 burst + 1 shock of 41 Joules
EGM layout
ventricular tachycardia with atrioventricular dissociation
at the end of duration, burst of 10 complexes at fixed rate
acceleration of arrhythmia into the VF zone
diagnosis of a VF episode and charging of capacitors
arrhythmia becomes polymorphic
shock of 41 Joules
arrhythmia termination
Take home message
there are 3 reasons why a shock may be delivered following the detection of an arrhythmia in the VT zone: 1) the electric shock is the first therapy programmed in the VT zone; 2) previous therapies (anti-tachycardia stimulation bursts) have proved ineffective; 3) an anti-tachycardia pacing burst accelerates the tachycardia into the VF zone, as in this example.
acceleration of VT and degeneration into VF are well-described complications following an anti-tachycardia pacing sequence, with an incidence of approximately 1 to 5% ; this justifies the absolute necessity of programming shocks as a back-up in the VF zone; the efficacy and safety of anti-tachycardia pacing are inversely related; a greater number of tachycardias can be terminated with a more aggressive protocol (shorter coupling intervals, more cycles per sequence, more sequences) but with an increased risk of acceleration
anti-tachycardia pacing can 1) accelerate a tachycardia with the same morphology as the previous one, 2) accelerate a tachycardia with a different morphology, or 3) cause an organized tachycardia to degenerate into VF.
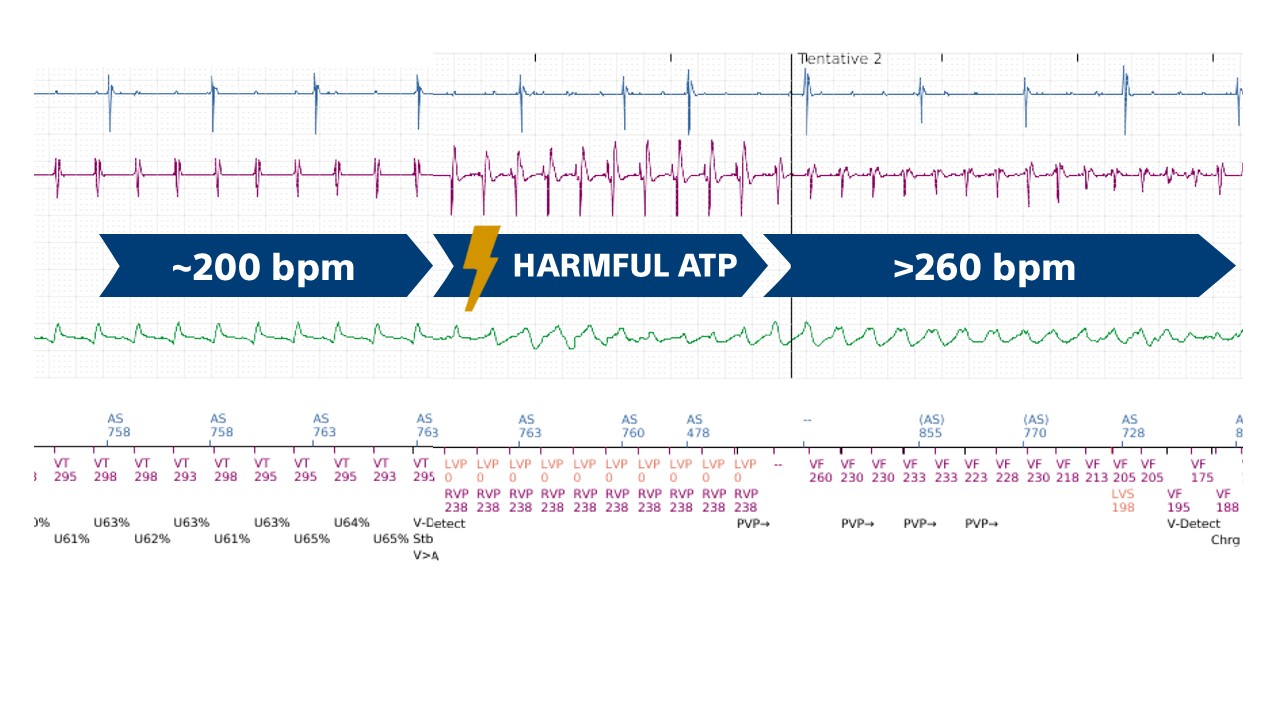
This figure shows how the anti-tachycardia pacing sequence accelerates a monomorphic VT at 200 beats/minute into a very rapid ventricular flutter and then into VF.