

Counters and detection zone
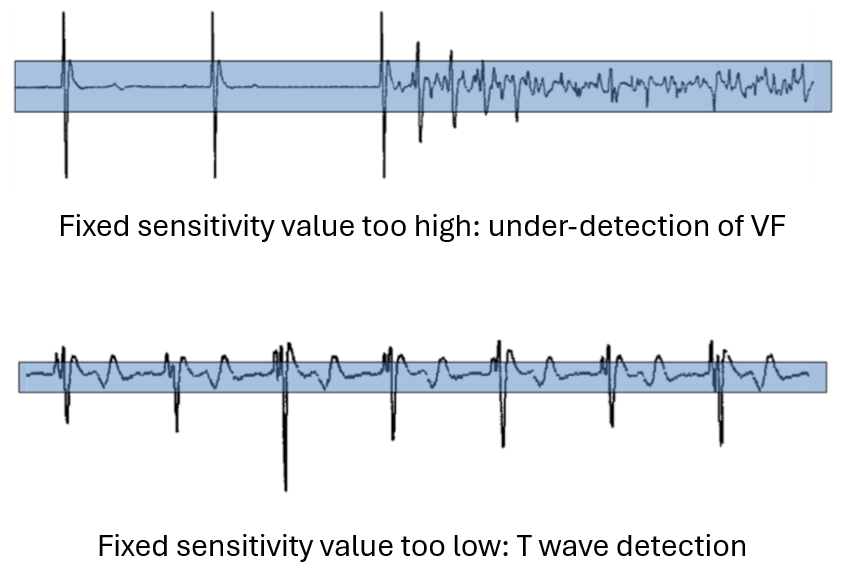
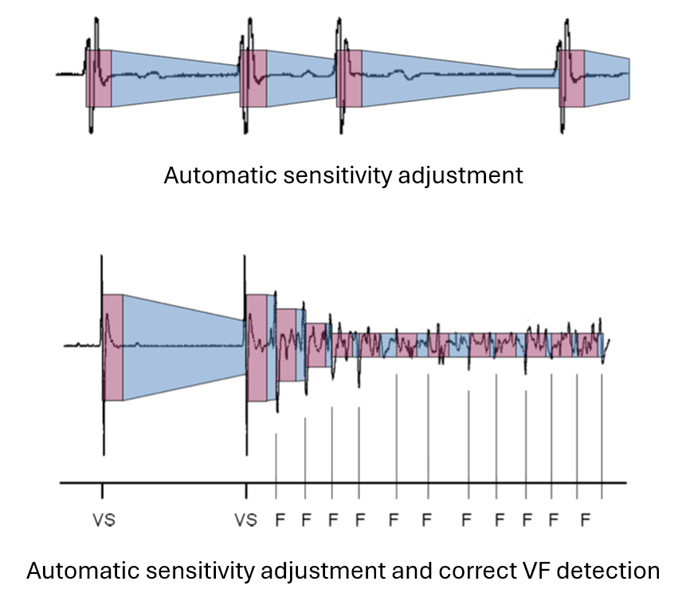
For a defibrillator to work properly, it must be able to detect the fast, low-amplitude signals characteristic of ventricular fibrillation, while not detecting cardiac signals other than QRS and extracardiac signals. This implies programming high sensitivity and short refractory periods. The detection threshold is not programmed to a fixed value, as in a pacemaker, but adapts automatically to the amplitude of the preceding R wave. Sensitivity then increases during the cycle, in order to search for any low-amplitude signals.
The detection circuit is blind during the post-detection ventricular refractory period, which is programmed to be short to avoid detecting the same depolarization several times, while still being able to detect a very rapid tachycardia. This refractory period is absolute for some manufacturers (blanking) or relative for others (possibility of searching for the maximum signal amplitude, but without the possibility of counting the same signal twice). At the end of this refractory period, the sensitivity adaptation level starts at a percentage of the detected R-wave amplitude, then gradually decreases until the programmed minimum value is reached. Each manufacturer has its own specificities regarding the value of the post-detection refractory period (more or less programmable), the starting value of sensitivity from R-wave detection, and the speed of sensitivity increase during the cycle.
Arrhythmia counting philosophies (number of cycles required to complete a VT or VF counter) differ between manufacturers and will be detailed in this chapter.
Choosing a defibrillator’s intervention frequency zones is an essential step in programming. Modern defibrillators allow the programming of several arrhythmia detection zones based on the RR intervals detected. Each zone can be specifically programmed for discrimination and therapy. The number of zones and the range of frequencies programmed should be adapted to the patient’s characteristics, history and indication for implantation.
In secondary prevention: in heart failure patients, the programming of frequency zones is adapted according to the VT cycle motivating implantation. In general, the lower limit of the VT zone is programmed 20 beats per minute slower than clinical VT, since antiarrhythmic treatment started or reinforced after implantation is likely to reduce VT frequency.
Primary prevention: in heart failure patients, the risk of developing ventricular tachycardia following implantation is substantial, and probably justifies programming 2 ventricular tachycardia detection and treatment zones in addition to the ventricular fibrillation zone. The main advantage of programming 2 separate ventricular tachycardia zones is to be able to specifically treat very rapid ventricular tachycardias, giving preference to painless anti-tachycardia pacing over electric shock. This has been demonstrated in the PAIN FREE I and PAIN FREE II clinical trials: anti-tachycardia pacing makes it possible to avoid 3 out of 4 shocks in the fast VT zone without significantly increasing adverse events. This leads to a significant benefit in terms of quality of life.
In a patient with complete atrioventricular block: the risk of inappropriate therapy for a supraventricular tachycardia is nil, which means that relatively low intervention frequencies can be set without altering specificity. Discrimination algorithms are unnecessary, since all spontaneous tachycardia is of ventricular origin.
In young, active patients: the risk of inappropriate treatment of physiological acceleration or conducted atrial fibrillation must be factored into the decision to program several intervention zones, trying to limit the overlap between the defibrillator’s intervention frequencies and the patient’s physiological frequencies.
In a patient with Brugada syndrome: the occurrence of organized ventricular tachycardia is extremely rare, whereas the risk of atrial fibrillation is increased. Programming a ventricular tachycardia detection and treatment zone in addition to the VF zone is therefore probably unnecessary or even dangerous. Programming an additional monitoring-only zone makes it possible to record any arrhythmias at lower frequencies and thus adapt programming. A single VF zone is usually programmed with a relatively high lower limit of this zone (frequency > 210-220 beats/minute).