patient with undefined defibrillation threshold
Tracing
Manufacturer Medtronic
Device ICD
Field Sensing
N° 10
Patient
A 56-year-old woman with ischemic cardiomyopathy, left ventricular ejection fraction of 20%, complete left bundle branch block and NYHA functional class III underwent implantation of a Medtronic InSync Sentry CRT-D for primary prevention, with VF induced at the end of the procedure.
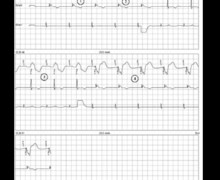
Graph and trace
- sinus rhythm (AS-BV);
- charge end (CE) of low energy shock;
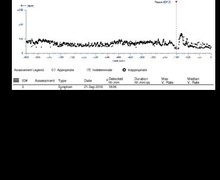
- induction of VF by T wave shock;
- VF correctly sensed by the CRT-D (FS and FD); capacitor charging (ventricular sensed events labeled VS);
- 25 J shock delivered (CD) after confirmation of the arrhythmia;
- ineffective shock with persistence of tachycardia, the ventricular signals are in the VF zone and labeled VS; some of the ventricular signals are not sensed.
- maximum 35 J shock delivered without reconfirmation of the arrhythmia by re-detection;
- restoration of sinus rhythm by successful shock (AS-BV).
Other articles that may be of interest to you


The verification of the efficacy of defibrillation may be of foremost importance at the time of the induction procedure. However, one must keep in mind the probabilistic behavior of the defibrillation process. Unlike the pacing threshold, the defibrillation threshold is not an absolute value, above which defibrillation is always successful and below which it is invariably ineffective. The aim of the induction at the end of the procedure is to ensure the presence of a safe margin relative to the maximum output of the device. The decision of changing the lead position should not rely only on the non-efficacy of a single shock. Indeed, even if the probability of success is 95% for a given shock amplitude, there still remains 5% risk of non success not meaning that the defibrillation threshold is high. In this particular patient, we re-checked an induction 5 minutes later with the same protocol (same shock amplitudes). During this second induction the first 25 J-shock did not terminate the arrhythmia. The ICD lead was initially positioned in a right ventricular basal position, the distal coil straddling the tricuspid valve annulus. This sub-optimal position of the lead may, at least partially, this non-efficacy. Repositioning of the lead to the septum resulted in reliable sensing and 2 consecutive successful 25 J shocks for induced VF, providing a sufficient safety margin.