Ventricular sensing during exercise
Tracing
Manufacturer Medtronic
Device CRT
Field Effort
N° 12
Patient
51-year-old man implanted with a triple-chamber defibrillator Consulta CRT-P for ischemic cardiomyopathy with left bundle branch block; excellent clinical response to resynchronization, a stress test (steps) is performed with the telemetry wand of the programmer placed over the device.
Graph and trace
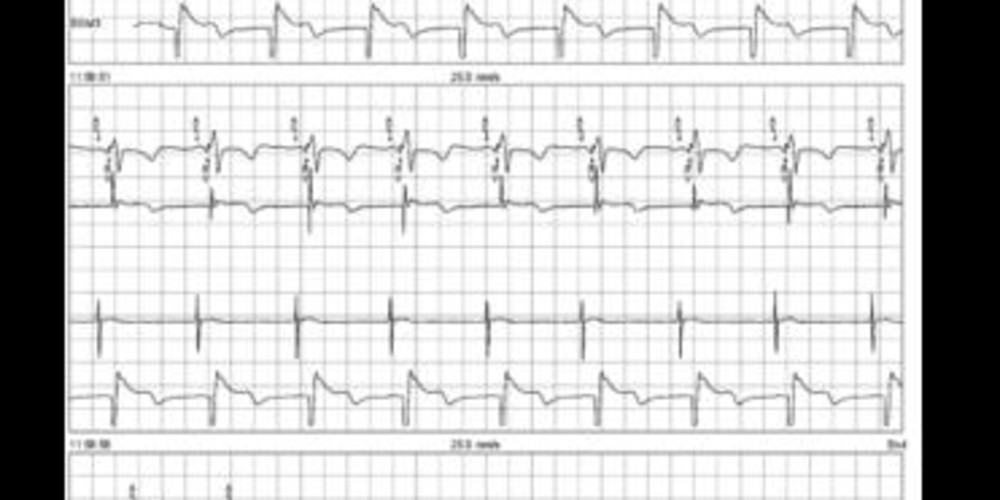
The first line corresponds to an electrocardiographic recording with superimposed markers, the second line corresponds to the bipolar RV EGM, the third line corresponds to the atrial EGM, the fourth line corresponds to the far-field EGM LV tip / RV ring - anode;
- sinus rhythm and biventricular pacing at rest (AS-BV);
- EGM recording obtained during the stress test, which explains the poor quality of the tracing; atrial rate at the maximum tracking rate; persistence of AS-BV cycles;
- acceleration of the atrial rate above the maximum tracking rate; discrete prolongation of the AV delay followed by a recovery of a spontaneous conduction and the loss of biventricular pacing (AS-VS cycles);
- stress test is stopped; persistence of AS-VS cycles;
- decrease of the heart rate below the maximum tracking rate and recovery of a biventricular pacing.
Other articles that may be of interest to you




In a CRT patient, the main objectives of a differential programming during exercise are to maintain a permanent and effective biventricular capture at high heart rates, to ensure a good contribution of atrial systole to cardiac output while maintaining atrioventricular synchronism, and to allow an appropriate acceleration of the heart rate which is the fundamental adaptive mechanism of cardiac output during exercise, particularly in heart failure patients.
The verification of maintained pacing and a permanent biventricular capture during exercise must be part of the standard assessment of a CRT patient. The recording of ventricular sensing episodes when occurring at high sinus rates should lead to suspect a loss of pacing during exercise. There are various possible causes for loss of biventricular pacing during exercise: atrial undersensing, frequent PVCs, sustained atrial or ventricular arrhythmias, shortening of PR interval during exercise below the programmed AV delay, programmed maximum tracking rate too low compared to the patient's capability. The conducting of an stress test allows to confirm the prerequisites of the proper functioning of the device during exercise, namely: good atrial sensing in patients without chronotropic incompetence, appropriate adaptive rate response in patients with chronotropic incompetence, that the 2:1 point is not reached during exercise (shortened AV delay and Auto PVARP), adequate setting of the maximum tracking rate and/or the maximum adaptive rate response, absence of arrhythmia during exercise (supraventricular arrhythmia, many PVCs, ventricular arrhythmia, pacemaker reentrant tachycardia).
The tracing recorded in this patient shows that during an exercise sinus tachycardia, the patient's heart rate exceeds the programmed maximum tracking rate. In a complete atrioventricular block patient, this would result in Wenckebach behavior. In this patient with preserved atrioventricular conduction, with no possible ventricular pacing beyond the maximum tracking rate, the AV delay is prolonged and spontaneous conduction reappears with loss of biventricular pacing at the peak of the exertion. An increase in the maximum tracking rate to 140 beats per minute eliminated this type of episode. This new programming was validated by the conducting of a new stress test which confirmed the persistent pacing and a biventricular capture to the maximum of the patient's capabilities. There is no reason to curb the programmed maximum tracking rate below the patient's acceleration capabilities during exercise. This type of episode is however very rarely symptomatic since it is not associated with a sudden drop in heart rate.