ventricular sensing failure
Tracing
Manufacturer Abbott
Device PM
N° 21
Patient
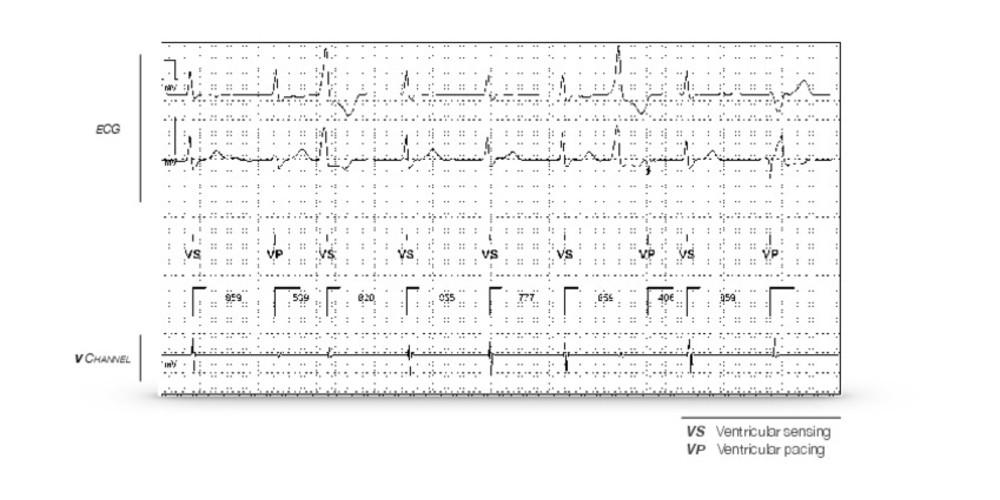
83-year-old man implanted with an AccentTM SR pacemaker for lipothemias due to slow AF; programming in VVI mode; consultation and recording of this tracing.
Graph and trace
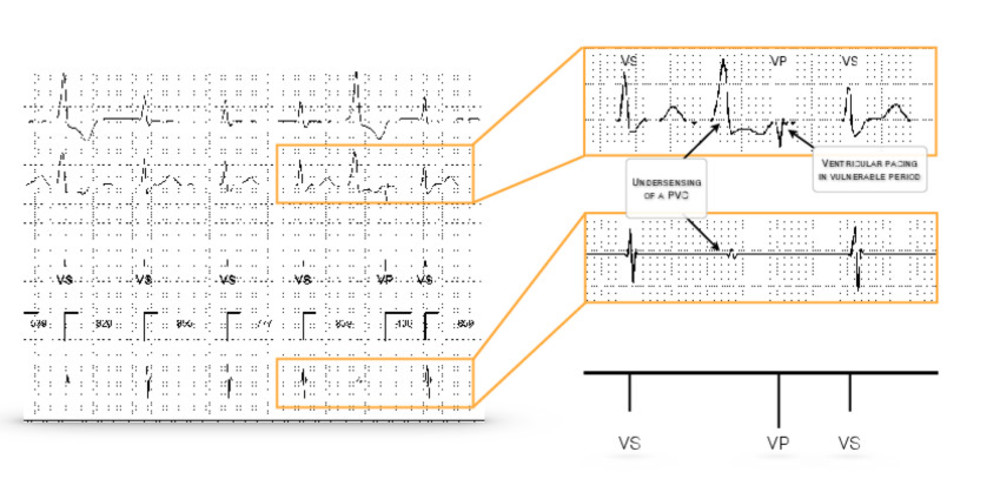
The pacemaker is programmed in VVI mode 70 beats/minute; patient in AF; the conducted QRS complexes are seemingly well detected; first premature ventricular contraction well detected; second unsensed premature ventricular contraction; ventricular pacing in vulnerable period without capture because occurring in the absolute refractory period of the ventricular myocardium.
Other articles that may be of interest to you

EGM recordings


This tracing shows the undersensing of a premature ventricular contraction causing pacing during the vulnerable ventricular period. The depolarization signal of an extrasystole is often fragmented with the slopes of its various components often being slower, thus increasing the risk of undersensing. In the absence of proper sensing, the pacemaker operates in asynchronous mode with no possibility of inhibition by intrinsic ventricular events. There is a low but non-zero theoretical risk of induction of a malignant polymorphic ventricular arrhythmia.
Sensitivity, expressed in millivolt (mV), defines the ability of the pacemaker to properly sense intrinsic cardiac events. Appropriate programming of the sensitivity level should allow the detection of all intrinsic cardiac events occurring in the implanted chamber while not sensing other events (crosstalk with sensing of cardiac signals from the other chamber, myopotentials, interference, etc). The programming of bipolar sensing allows enhancing the specificity of detection relative to unipolar sensing by limiting the risk of sensing extracardiac signals or crosstalk while enabling the programming of high sensitivity values. On the other hand, in unipolar configuration, the risk of crosstalk or sensing extracardiac signals requires the programming of a lower sensitivity level with an increased risk of undersensing.
Traditionally, unlike implantable defibrillators, pacemakers functioned with a fixed and stable sensitivity throughout the cardiac cycle. Nowadays, the various manufacturers offer in their range of devices a fusion between the respective operating platforms of pacemakers and defibrillators. Although the sensing constraints are not the same (critical necessity for a defibrillator to detect and treat very rapid, polymorphic and low-voltage ventricular rhythm disorders), modern pacemakers allow programming an adaptive sensitivity (variable sensitivity level according to the amplitude of the R wave or the sensed P wave). The principle of automatic sensitivity control is to adjust the sensitivity level according to the amplitude of the P wave or the previous R wave and subsequently increase the sensitivity during the cycle. For AbbottTM pacemakers, in bipolar sensing, atrial and ventricular sensitivity can be programmed to automatic (AutoSenseTM or SenseAbilityTM) or fixed. Conversely, the sensitivity is necessarily fixed if sensing is unipolar. When the lead is coded as bipolar, it is possible to program unipolar sensing either between the distal end and the can or between the ring and the can. In the presence of an oversensing or undersensing problem, the choice of the sensing method (fixed or adaptive) will depend primarily on the amplitude of the signals and the variability of the amplitude of these signals.
When an adaptive ventricular sensitivity is programmed, the sensitivity is automatically adjusted to a percentage of the largest value of the 2 components of the previously sensed signal (positive or negative). After sensing of an R wave, at the end of the refractory period, the sensitivity adjustment level begins at a (programmable) percentage of the sensed R wave amplitude (without exceeding 6 mV nor falling below 1 mV), remains the same during the adjustment delay (programmable) after which the sensitivity gradually increases until reaching the programmed sensitivity value. The following parameters are programmable: the post-sensed adjustment level (threshold start between 50 and 100%), the post-paced adjustment level (Auto or between 0.2 and 3 mV), the post-sensed decay delay (between 0 and 220 ms), the post-paced decay delay (Auto or between 0 and 220 ms) and the maximum sensitivity (between 0.2 mV and 2 mV). When the ventricular post-paced decay delay is set to Auto, the device automatically adjusts the delay used after ventricular paced pulse to compensate for the shortening of the QT interval associated with fast pacing rates.