Displacement of the atrial lead into the ventricle
Tracing
Manufacturer Biotronik
Device PM
Field Pacing
N° 17
Patient
74-year-old man implanted with an Evia DR-T dual-chamber pacemaker for atrioventricular block; interrogation of the pacemaker the day after implantation.
Graph and trace
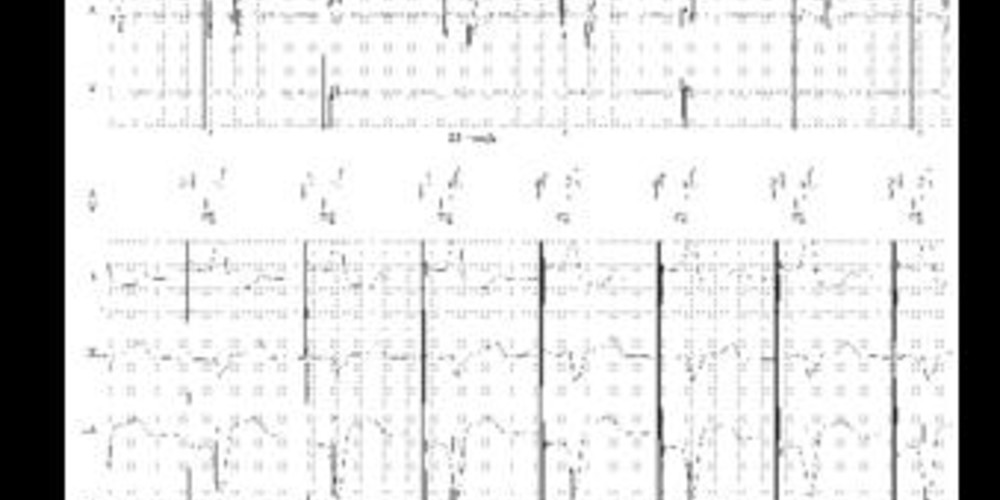
Tracing 17a
- atrial pacing and ventricular pacing; sensing of a signal in the atrial channel in the far-field protection (FFP) period;
- atrial pacing and probable ventricular capture (identical pattern to the previous QRS); ventricular depolarization is detected by the ventricular channel in the safety window; pacing at the end of the safety window without capture;
Tracing 17b
Reprogramming in DDI mode 50 bpm;
- no sensing of sinus activity; sensing of spontaneous ventricular activity by the atrial channel and the ventricular channel (quasi-simultaneous sensing).
Patient: 60-year-old man implanted with an Evia DR-T pacemaker for paroxysmal atrioventricular block; 3 months after implantation, transmission of a periodic EGM by telemedicine.
Tracing 17c
Normal
- ventricular sensing classified as PVC (not preceded by atrial activity classified as AS); sensing of a signal concurrent with ventricular sensing in the atrial channel (in the far-field protection period);
Encouraged sensing
- no modification of the tracing;
Encouraged pacing
- atrial pacing with probable ventricular capture; ventricular sensing and pacing at the end of the safety window (100 ms after atrial pacing) without capture;
Pulmonary radiography reveals a displacement of the atrial lead in the ventricular chamber.
Other articles that may be of interest to you


These different tracings correspond to an early dislodgement of the atrial lead that has fallen into the ventricle. On the first tracing, the atrial lead drives the ventricle intermittently. On the second tracing, a slowing of the minimum rate allows highlighting the sensing of ventricular depolarization by the atrial lead. A repositioning of the atrial lead enabled the resumption of normal operation. The third tracing illustrates the value of the transmission of a periodic EGM enabling to make the diagnosis in this asymptomatic patient. One of the interesting features of the BiotronikTM devices is to approximate, during this periodic EGM, what is actually performed during the consultation, with transmission of a real-time EGM without modification of the programming (Normal), followed by transmission of an EGM with reduction in pacing rate in order to favor spontaneous activation and verify the quality of the sensing (Encouraged sensing), and lastly, transmission with an increase in pacing rate in order to favor pacing and verify the effective capture.
When an abnormal tracing is revealed in the immediate aftermath of implantation of a dual-chamber pacemaker, the diagnosis of lead dislodgement should be evoked when the functioning of a single lead appears abnormal. Inverting the 2 leads seems more likely when the lead connected to the atrial channel senses and/or paces the ventricle and the lead connected to the ventricular canal senses and/or paces the atrium.