Sensing optimization and diagnosis of atrial fibrillation
Tracing
Manufacturer Medtronic
Device PM
Field Management of atrial arrhythmias
N° 30
Patient
77-year-old man implanted with an Adapta dual-chamber pacemaker for complete atrioventricular block; routine consultation.
Graph and trace
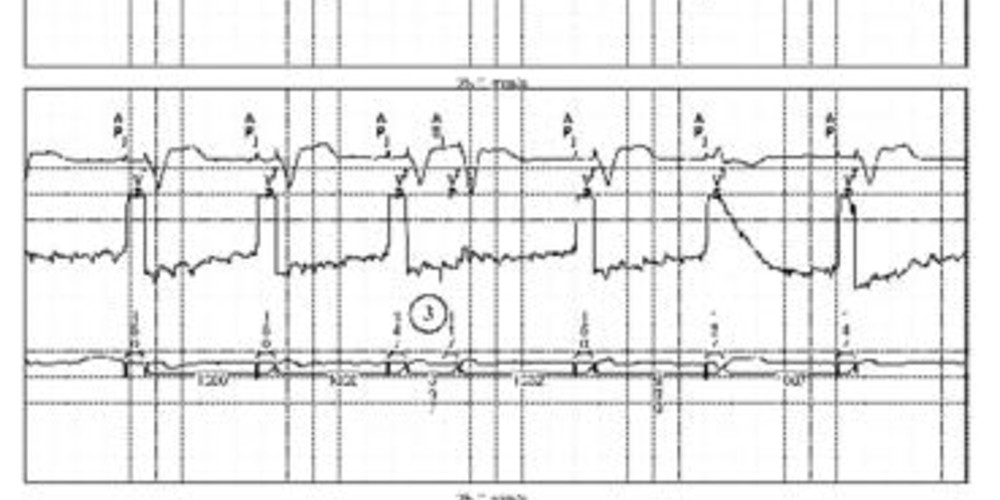
Tracing 30a: the first line corresponds to lead II with the superimposed markers, the second line to the atrial EGM, the last line to lead I with the superimposed intervals;
- atrial and ventricular pacing (AP-VP);
- the atrial EGM reveals the presence of small-amplitude atrial signals not sensed by the device; this explains the atrial pacing (AP);
- one of the signals of slightly greater amplitude is sensed then followed by an AV delay and a ventricular pacing;
Trace 30b: atrial sensing is initially programmed to 0.5 mV; optimization of sensing at the maximum capacity of the device;
- same tracing as previously;
- change in the programming of atrial sensing;
- improved atrial sensing and mode switching (MS);
- progressive slowing of ventricular pacing.
Other articles that may be of interest to you
EGM recordings
EGM recordings

The ventricular runaway observed during a rapid atrial rhythm can only occur if the atrial signals are detectable. In the presence of permanent atrial arrhythmia undersensing and a complete atrioventricular block, the behavior of the pacemaker is of the DVI-type, with AV pacing at the base rate or current rate responsive frequency. Atrial pacing is unnecessary and energy intensive. In addition, the system is unable to memorize the episode which can therefore go unnoticed if the patient is asymptomatic. When the atrial signals are sensed intermittently, ventricular rhythm becomes erratic.
In this patient, an increase in atrial sensitivity enables a correct diagnosis of the arrhythmia with switching from DDD mode to DDIR mode. In MedtronicTM pacemakers, the rate response is systematically programmed during a mode switching even if the initial mode was not rate responsive. This appears appropriate in this patient with complete atrioventricular block and without possibility of chronotropic adaptation when the patient is in atrial fibrillation.