Blanked flutter
Tracing
Manufacturer Medtronic
Device PM
Field Management of atrial arrhythmias
N° 31
Patient
57-year-old woman with pulmonary arterial hypertension under anticoagulant and amiodarone therapy for episodes of paroxysmal AF, implanted with a dual-chamber pacemaker for episodes of syncope due to paroxysmal atrioventricular conduction disorder; hospitalization for cardiac decompensation with palpitations since 2 weeks.
Graph and trace
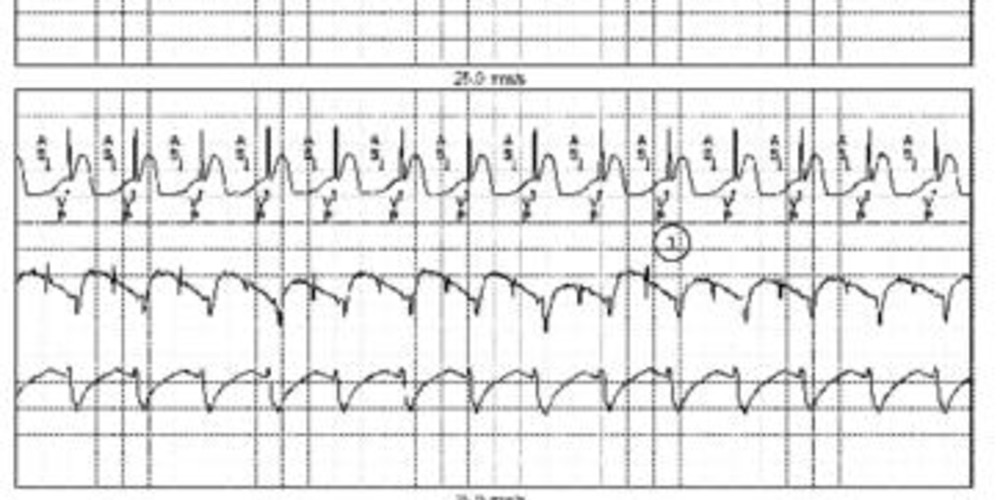
Tracing 31a: the first line corresponds to lead I with the superimposed markers, the second line to the atrial EGM and the last line to the ventricular EGM;
- rapid atrial rhythm around 130 beats/minute (maximum synchronous rate programmed at 140 beats/minute) followed by 1/1 ventricular pacing;
Tracing 31b: pacemaker interrogation shows that the blanked flutter search algorithm is deprogrammed; programming of this algorithm;
- continuation of the fast AS-VP rhythm;
- programming of the blanked flutter search algorithm (successful programming);
- during 8 consecutive intervals, the AA interval is less than twice the AV delay + post-ventricular atrial blanking (this sum corresponds to the total atrial blanking) and less than twice the interval of the programmed sensing rate: suspicion of 2/1 flutter; on the ninth interval, the device prolongs the PVARP; the event previously labeled AS is now labeled AR and is not followed by ventricular pacing; the ensuing atrial event, which was hitherto hidden in the post-ventricular atrial blanking, is visualized in the absence of ventricular pacing and labeled AS; diagnosis of blanked 2/1 flutter;
- mode switching (MS) to DDIR mode;
- progressive reduction of the ventricular pacing rate;
- reappearance of spontaneous ventricular rhythm;
Tracing 31c: the 12-lead electrocardiogram is indicative of a common flutter;
- persistence of this atrial flutter pattern with variable ventricular conduction;
Tracing 31d: the patient underwent a well conducted anticoagulant treatment; attempted termination by rapid pacing of the atrium with the aid of the pacemaker;
- rapid atrial pacing burst; the duration of the burst (2 to 3 seconds) and the pacing rate (slightly faster than the flutter rate) are set by the cardiologist;
- failure of the burst and persistence of the same arrhythmia;
Tracing 31e: renewed attempt at termination;
- new burst faster than the preceding burst;
- degradation of the arrhythmia into atrial fibrillation; the auriculograms are faster and irregular both in rhythm and morphology.
Other articles that may be of interest to you




The initial absence of fallback on this episode of undiagnosed flutter was hence responsible for a prolonged rapid ventricular pacing favoring cardiac decompensation. Indeed, this patient experienced palpitations for almost 2 weeks, day and night. The programming of the blanked flutter search algorithm allowed terminating this inappropriate pacing and the return to a more acceptable ventricular conduction rate. The attempt to terminate this arrhythmia could only be achieved because the effective anticoagulation conditions were met (INR > 2 for more than 3 weeks). Pacing above the flutter rate proved ineffective. Acceleration of the pacing did not allow a return to sinus rhythm although degraded the arrhythmia into atrial fibrillation. This patient showed spontaneous termination a few minutes after pacing. It is common that, once installed, an atrial flutter can persist for long periods of time. An attempt at termination can lead to immediate success with a return to sinus rhythm but also to a more delayed success with, in the first stage, a transformation of the arrhythmia into AF followed secondly by termination.
The blanked flutter algorithm is no longer present on the new dual-chamber pacemaker platforms. Indeed, as explained previously, it is now possible to program the blanking to partial or partial + which enables atrial sensing in this phase following ventricular pacing and which considerably limits the risk of not sensing 1 out of 2 atrial activities. However, regardless of the programming, there is an absolute blanking of 30 ms to avoid sensing of the pacing spike (very limited risk that an atrial activity is contemporaneous with this spike).