Oversensing of P wave during atrial arrhythmia
Tracing
Manufacturer Boston Scientific
Device ICD
Field Sensing
N° 5
Patient
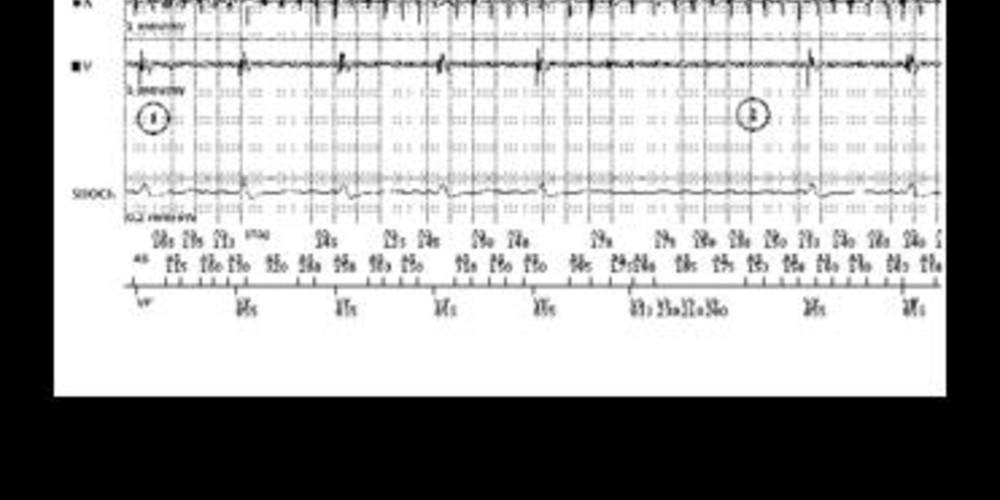
This 53-year-old man underwent implantation of a Boston Science Teligen dual chamber defibrillator in the context of dilated cardiomyopathy and complete atrioventricular block with integrated bipolar ventricular lead (the anode of the sensing circuit is the defibrillating electrode of the RV lead). He complained of recurrent light-headedness; an alert was received by the Latitude remote monitoring center.
Graph and trace
Tracing
- atrial fibrillation accurately detected by the defibrillator and rate responsive ventricular pacing (VP-Sr) in this pacemaker-dependent patient; the device has switched to VVIR mode;
- oversensing at the level of the ventricular sensing channel; the high-voltage channel recording confirmed that no ventricular arrhythmia was on-going. A rapid atrial activity is visible at the level of the ventricular sensing channel; 3 short, consecutive ventricular cycles were detected, explaining the storage of this episode in the memories and its transmission by remote monitoring; this oversensing caused a nearly 3-second pause responsible for the patient’s presenting symptoms;
- end of oversensing.
Other articles that may be of interest to you



Oversensing of the atrial activity occurs preferentially when the defibrillating electrode of an integrated bipolar lead is straddling the tricuspid valve. This patient presented with complete atrioventricular block. Oversensing of the atrial arrhythmia by the ventricular channel caused a pause, as the oversensed rapid rhythm inhibited ventricular pacing. This patient presented with recurrent light-headedness due to these episodes. A first remedial choice consists of lowering the ventricular sensitivity to prevent oversensing of the atrial activity. This programming might, however, be associated with a risk of a true VF undersensing. A new induction of VF would be required to confirm the reliable detection with the programming of this new sensitivity value. A second option is to plan the repositioning of the lead. In this patient, this option was favored, and a bipolar lead was re-implanted in the high septum, with placement of the entire coil in the distal ventricular cavity.