Induction with high defibrillation threshold
Tracing
Manufacturer Boston Scientific
Device ICD
Field Implantation
N° 3
Patient
This 57-year-old man underwent implantation of a Boston Science Teligen single chamber defibrillator for secondary prevention of sustained VT, in the context of hypertrophic cardiomyopathy. VF was induced at the end of the procedure. The device was programmed to deliver a first 17 J shock, a second 26 J shock, followed by 6 shocks at the maximum strength of 41 J.
Episode summary
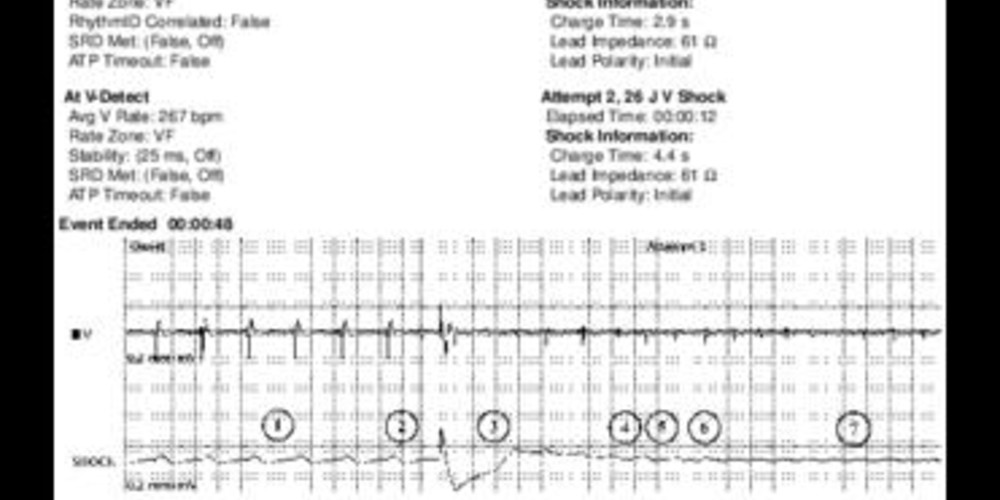
After the induction of VF, 2 shocks of increasing strength (17 and 26 J, respectively) were delivered; the initial polarity of both shocks was cathodal (the RV coil serving as the cathode for the first phase).
Graph and trace
Tracing
- 8 stimuli at a rate of 150 bpm;
- low-amplitude (1.1 Shk) shock delivered on the T wave;
- after the refractory period, the first ventricular event (--) was not counted;
- a polymorphic ventricular tachyarrhythmia alternating initially between sinus (VS) and VF (VF) zones was triggered;
- the initial rolling detection window began only after the detection of 3 short consecutive cycles. In this case, the first 2 short cycles (VF) were followed by 1 VS. Consequently, the 3 short consecutive cycles were missing and the initial detection window did not begin;
- third consecutive cycle in the VF zone;
- after 8 cycles in the VF zone (including the first 3 consecutive cycles) with 2 interposed VS cycles, (fulfilling the of 8 out of 10 criterion), an episode of VF (V-Epsd) was detected;
- the first cycle following the end of the Duration (1 sec) is a VS, explaining the presence of the “V-Dur” marker (while the 6 out of 10 criterion remains fulfilled, the V-detect marker can only appear after a short cycle;
- on the first VF cycle following the end of the Duration (with the 6 out of 10 short cycles criterion remaining fulfilled), a sustained episode was detected, explaining the “V-detect” marker; onset of the capacitors charge;
- end of charge;
- re-confirmation at the end of charge: the next first cycle following the charge was not counted (--), the next 2 were in the VF zone, fulfilling the 2 out of 3 short cycles criterion;
- delivery of a 17 J electrical shock;
- refractory period following the shock; the first ventricular cycle that followed was not counted;
- the electrical shock was unsuccessful and the arrhythmia continued. After an electrical shock, a re-detection phase begins, applying the same criteria for ventricular detection from earlier;
- from this cycle onward, the 8 out of 10 short cycles criterion was fulfilled (no visible marker on the tracing); onset of the post-shock Duration (1 sec);
- re-detection of VF (8 out of 10 cycles in the VF zone + 1 sec post-shock Duration) and repeat charge of the capacitors;
- end of charge;
- re-confirmation: the first cycle after the charge was not counted (--); the next 2 cycles were in the VF zone; the of 2 out of 3 short cycles criterion was fulfilled; a 26-J electrical shock was delivered;
- a 500-ms refractory period followed the shock; the next ventricular cycle was not counted;
- the electrical shock was unsuccessful and the arrhythmia continued;
- artifact caused by the shock delivered by the external defibrillator (ordered by the operator);
- termination of the arrhythmia and several ventricular paced events.
Graph
The graph illustrates a few undersensed R waves (23) and shows the delivery of 2 unsuccessful electrical shocks (24 and 25).
Other articles that may be of interest to you



In this patient, the first shock was programmed at a relatively low value of 17 J. When the operator became aware of its failure, he ordered the charge of the external defibrillator in order to not delay the therapy, as soon as the second shock delivered by the implantable defibrillator was also unsuccessful. The lead that had been implanted initially at the RV apex was repositioned to the septum. However, defibrillation remained unsuccessful despite this new lead location. A coil was then added in the coronary sinus and a new induction procedure was performed in search of a better safety margin (31 J shock, i.e. a 10 J margin with respect to the maximum device output capability). This new shock vector was associated with successful defibrillation.