SecureSense™ algorithm and loss of RV capture
Tracing
Manufacturer Abbott
Device ICD
Field Securesence
N° 11
Patient
This 76-year-old man received a Abbott Ellipse™ DR defibrillator for the management of an ischemic cardiomyopathy with a long PR interval on the electrocardiogram. A non-sustained episode of noise on the ventricular lead was retrieved from the device memory.
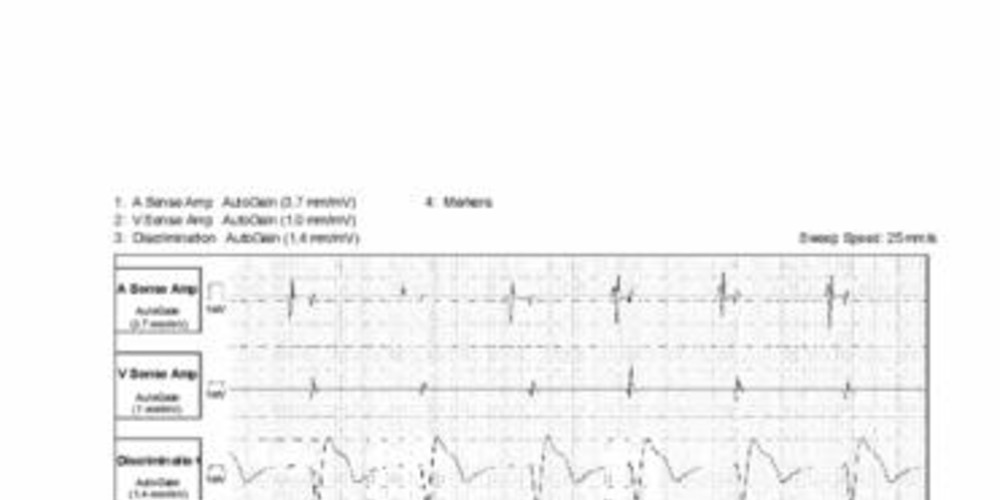
Graph and trace
- ventricular pacing and probable absence of capture (absence of ventricular depolarization on the discrimination channel); AV conduction with a prolonged PR interval and sensing of spontaneous ventricular activity on the bipolar channel (short cycles, -);
- same sequence with second short cycle; activation of the noise counter 350 ms after this second short cycle;
- same sequence; the spontaneous QRS is sensed on the discrimination channel and marked VS2;
- the noise counter is at 5, the VT or VF counter is not filled; diagnosis of non-sustained noise of ventricular lead (NSLN); the number 5, and the terms non-sustained noise ventricular lead, NSLN, date from old models. With the more recent models, a noise counter at 10 is needed to record an episode, and the terms applied are: diagnosis of non-sustained ventricular oversensing and SNS.
Other articles that may be of interest to you




The activation of the SecureSense™ algorithm makes diagnoses that are sometimes unexpected as, in this case, the intermittent loss of RV capture. In this patient, the programmed amplitude of stimulation was too low, at the limit of threshold and without safety margin. With each loss of capture, a SecureSense™ alert was recorded. The delay between the ineffective ventricular stimulus and the sensing of spontaneous conducted activation was longer than the post-pacing ventricular blanking period and was expressed by the detection of a short cycle on the bipolar channel. Conversely, the spontaneous ventricular event was the only event sensed on the discrimination channel, explaining the absence of short cycle (no ventricular depolarization after the ventricular stimulus). An adapted programming of the stimulation amplitude solved the problem.