Lead to lead interaction and inappropriate therapies
Tracing
Manufacturer Abbott
Device ICD
Field Sensing
N° 8
Patient
Young patient implanted with a single lead Abbott ICD (Fortify Assura). Exteriorization of the device and partial extraction of the RV lead (persistence of the 5 cm distal portion of the lead). Implantation of a new integrated bipolar lead. Consultation for repeated shocks.

Graph and trace
Episodes summary
Multiple episodes diagnosed VF by the device and delivery of 22 shocks in 13 minutes.
Narrative 1
Episode of VF requiring 1 high-amplitude shock.
Tracing
- sinus rhythm;
- polymorphic ventricular arrhythmia with signals sensed in both the near and far-field channels; VS2 in the discrimination channel after 2 cycles classified VF;
- detection of VF episode (12 F classified cycles) and start of the capacitors charge; the SecureSense algorithm does not withhold therapy (arrhythmia appropriately detected in both channels);
- end of charge;
- delivery of the high amplitude shock on the second fast cycle (F);
- return to sinus rhythm after 5 consecutive VS;
Narrative 2
Episode of VF (a few minutes after the previous one) requiring 1 high-amplitude shock.
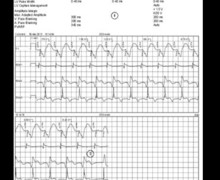
Tracing
- oversensing of signals in both the near-field and far-field (discrimination) channels;
- VVI episode pacing mode after 4 F classified cycles;
- detection of VF episode (12 F classified cycles) and start of the capacitors charge; the oversensing being present in both channels, the SecureSense algorithm does not withhold the therapies;
- end of charge;
- delivery of the high amplitude shock on the first fast cycle (F);
- return to sinus rhythm after 5 consecutive VS;
Other articles that may be of interest to you



This patient presented initially with a true episode of fast ventricular arrhythmia requiring appropriate delivery of a shock. The functioning of the SecureSense algorithm was correct (no inhibition of the therapies during VT or VF). The second episode was related to a lead-to-lead interaction (chatter), the retained fragment being in intermittent contact with the distal coil of the RV lead during heart contraction explaining the oversensing. Both the RV sensing channel (tip to coil, integrated bipolar sensing) and the discrimination channel (coil to can) incorporated the coil in the sensing circuit explaining why the oversensing was present in these 2 channels and why the SecureSense algorithm did not prevent the occurrence of inappropriate therapy. The retained fragment was extracted with a snare through femoral approach.