Bipolar LV lead threshold test
Tracing
Manufacturer Medtronic
Device CRT
Field Left ventricular pacing
N° 3
Patient
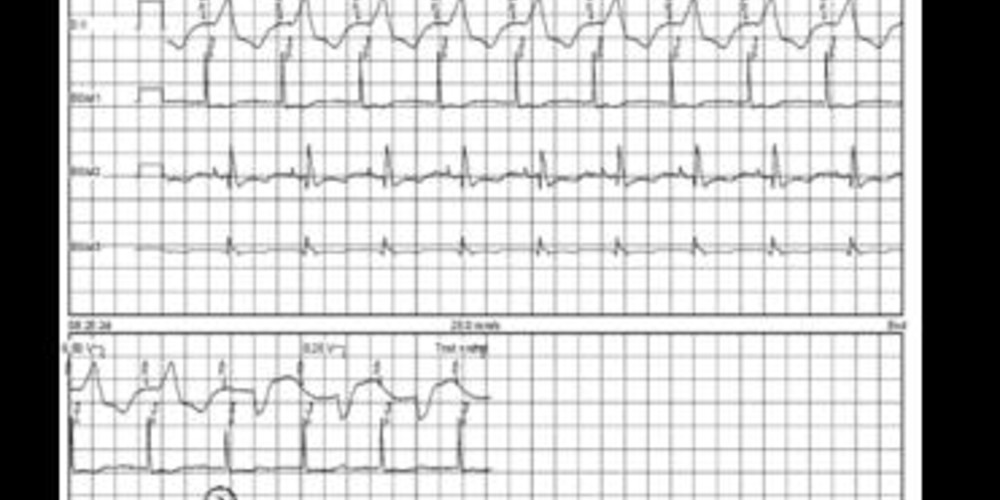
70-year-old man implanted with a triple-chamber defibrillator Viva XT CRT-D and a Medtronic 4194 LV lead for ischemic cardiomyopathy with a left bundle branch block; follow-up 3 days after implant; LV threshold performed in various pacing configurations (pacing DDD 90 bpm, amplitude decrement, fixed pulse width of 0.4 ms).
Graph and trace
- LV threshold in LV tip – RV coil configuration;
- loss of LV capture at 0.5 V (threshold 0.75 V/0.4 ms); absence of phrenic nerve stimulation;
- LV threshold in LV tip – LV ring (anode) configuration;
- loss of LV capture at 0.5 V (threshold 0.75 V/0.4 ms); absence of phrenic nerve stimulation;
- LV threshold in LV ring – LV tip configuration;
- loss of LV capture at 2V (threshold 2.25 V/0.4 ms); absence of phrenic nerve stimulation;
- LV threshold in LV ring – LV tip;
- loss of LV capture at 3V (threshold 3.25 V/0.4 ms); absence of phrenic nerve stimulation.
Other articles that may be of interest to you




In a patient implanted with a MedtronicTM triple-chamber defibrillator connected to a bipolar left ventricular lead, 4 left ventricular pacing configurations can be programmed: LV tip – RV coil, LV tip – LV ring (anode), LV ring –RV coil, LV ring – LV tip. Various elements can more or less influence the choice of programming to privilege: presence of diaphragmatic pacing, hemodynamic impact, pacing threshold and impedance. The selected left ventricular pacing configuration must enable effective and permanent capture by maintaining sufficient safety without stimulation of the phrenic nerve, while limiting the energy used in order to increase the longevity of the device. In this patient, the left ventricular lead was positioned in an anterolateral vein and no configuration was associated with phrenic stimulation even for large amplitudes. On this type of left ventricular lead, both electrodes are in proximity to each other, which explains an identical electrocardiographic pattern (confirmed on a 12-lead ECG) regardless of the selected configuration. It would thus seem logical to think that the selected configuration will have little influence on hemodynamic impact. The choice of the configuration to be privileged therefore did not depend on these first two parameters. On the other hand, the pacing threshold differed substantially according to the selected configuration. When the distal electrode served as the cathode (LV tip – RV coil and LV tip – LV ring), the pacing threshold was less than 1 volt for 0.4 ms. Conversely, when the proximal electrode served as the cathode (LV ring – LV tip and LV ring – RV coil configurations), the pacing threshold was higher (> 2 volts for 0.4 ms). This difference is frequently observed, the 4194 lead having an anode ring of large surface area which decreases current density at the edges of the electrode thereby increasing the threshold. The choice of configuration in this patient will therefore have a significant influence on the delivered amplitude necessary for obtaining a sufficient margin and hence have a major influence on energy consumption and on the lifespan of the device. The fourth parameter to be integrated in the decision process is the pacing impedance value. All things being equal, it is preferable to program the pacing configuration which offers the highest impedance, since the energy consumed by the device is inversely proportional to the value of the impedance. When the LV threshold is high, it is important to take this parameter into account.