Induction of ventricular fibrillation with sensing defects
Tracing
Manufacturer Abbott
Device ICD
Field Implantation
N° 4
Patient
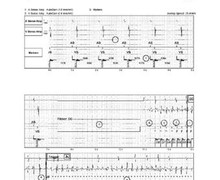
A 47-year-old man presenting with hypertrophic cardiomyopathy and complete atrioventricular block after septal embolization, received a dual chamber Atlas ICD for secondary prevention of ventricular tachycardia (VT).
Main device programming (during the induction procedure)
- Single VF zone for rates >187 bpm
- 12 cycles in the VF zone were needed for the diagnosis
- Sensitivity programmed at 0.3 mV
- First shock at 22.5 J, second shock at 36 J (maximum strength).

Graph and trace
- Sinus rhythm and ventricular pacing (AS-VP);
- Delivery of DC for 2 sec;
- Blanking phase for 600 ms;
- Induction of fast and polymorphous ventricular arrhythmia;
- Failure of ventricular sensing; the first sensed signal is of high enough amplitude, though the second is not sensed. Ventricular sensing depends on both the amplitude and the slope of the analyzed electrogram (EGM), as well as on the amplitude of the previous EGM. The amplification of the ventricular channel was 1 mm/mV, which facilitated the analysis of the tracing. Only the positive or the negative deflexion (the tallest) of the ventricular EGM is measured. On this tracing, marked variations in the amplitude as well as very low amplitude EGM are present, both of which promote undersensing;
- This ventricular EGM was not classified, because of discordance between the value of the on-going cycle, which was outside the VF zone, and the average of the 3 previous cycles plus the on-going cycle, which was inside the VF zone;
- Prolonged failure of ventricular sensing;
- Detection of a VF episode (Trigger) and start of the capacitors charge (asterisks);
- Another failure of sensing ventricular EGM of low amplitude during the charge;
- End of charge;
- No shock could be delivered on the cycle that followed the charge; despite undersensing, the cycles were classified in the VF zone;
- Delivery of 656 V (22.5 J) shock; in the wake of the shock, a 1-sec blanking period prevented any sensing and a 2-sec period prevented any pacing, explaining the delay before the onset of VP (in DDI mode, which was the episode pacing mode);
- Successful shock and diagnosis of return to sinus rhythm after 5 consecutive VP or VS cycles; the DDI post-choc pacing mode continued for 30 sec after the diagnosis of return to sinus rhythm.
Other articles that may be of interest to you



During the induction test, ventricular sensing is usually set at the highest possible value (1 mV) in order to place the system in adverse sensing conditions and render the test as insensitive as possible. A proper detection of VF at this high value suggests the presence of a wide safety margin with the system programmed at the nominal value of 0.3 mV on the long term. In this patient and for this test, however, the sensitivity was programmed at 0.3 mV, and flaws in ventricular sensing were noted during the induction. Induction tracings must be meticulously scrutinised in order to detect these sensing failures, which may be subtle and challenging to diagnose, as they delay the delivery of shocks only slightly. Sensing failures are facilitated by wide variations in the signal amplitude, which mislead the automatic control of the sensitivity. The failure of sensing low-amplitude VF EGM occurs after the occurrence of a signal of greater amplitude. In this patient, the ventricular sensitivity programmed for the test was 0.3 mV, and ventricular sensing during sinus rhythm, measured at 4.1 mV, was moderately reliable. The decision was made, consequently, to relocate the lead from the right ventricular (RV) apex toward the high septum, where sensing was reliable. A repeat induction procedure confirmed that VF was properly detected and defibrillation was successful.