Rate limitation and Quick Convert algorithm
Tracing
Manufacturer Boston Scientific
Device ICD
N° 8
Patient
This 32-year-old man presenting with hypertrophic cardiomyopathy underwent implantation of a single chamber Boston Science Teligen defibrillator for management of VT associated with syncope. He was seen for the complaint of palpitation and near syncope followed by the delivery of an electrical shock.
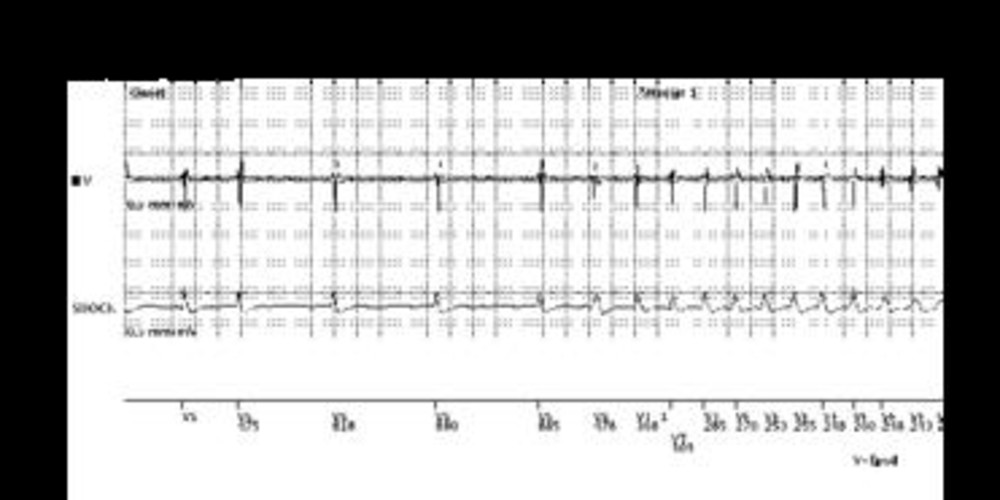
Graph and trace
- sinus rhythm;
- VES;
- tachycardia initially detected in the VT-1, then in the VT, then in the VF zone. The monomorphic aspect of the tachyarrhythmia on the detection as well as on the high-voltage channels was consistent with probable VT detected in the VF zone;
- initial 8 out of 10 detection criterion fulfilled for the VT-1 zone; onset of the initial VT-1 zone Duration;
- initial 8 out of 10 detection criterion fulfilled for the VT zone; onset of the initial VT zone Duration;
- initial 8 out of 10 detection criterion fulfilled for the VF zone; onset of the initial VF zone Duration;
- end of the VF zone Duration; the ventricular rate (an average of the last 4 cycles) was >250 bpm. Consequently, the Quick Convert burst was not delivered;
- onset of the charge without delay;
- end of the charge;
- 41-J electrical shock delivered after the confirmation phase;
- successful electrical shock and termination of the arrhythmia.
Other articles that may be of interest to you



The current consensus is to treat organized ventricular tachyarrhythmias by ATP instead of electrical shocks. This is because a large proportion of episodes at rates >200 bpm, diagnozed as VF by the defibrillator, actually consist of rapid monomorphous VT, which can be successfully ended by programmed ventricular stimulation. Since ATP is painless, lowers the energy consumption and spares the batteries, it must be given priority as first-line therapy for organized ventricular rhythms, even when they are very rapid. However, the delivery of an electrical shock is sometimes inescapable. In this patient, rapid, monomorphic VT was detected in the VF zone and treated outright with an electrical shock of maximum strength. A non-programmable rate limit of ≤250 bpm for the delivery of Quick Convert bursts of ATP has been assigned to this type of defibrillator. This limit prevents the delivery of ATP for non-physiologic, often very rapid pseudo-tachycardias observed with lead fractures or with P, R or T wave oversensing.