Automatic right ventricular threshold measurement
Tracing
Manufacturer Biotronik
Device PM
Field Pacing
N° 20
Patient
69-year-old man implanted with an Evia DR-T dual-chamber pacemaker for paroxysmal atrioventricular block; during the consultation, automatic right ventricular threshold measurement.
Graph and trace
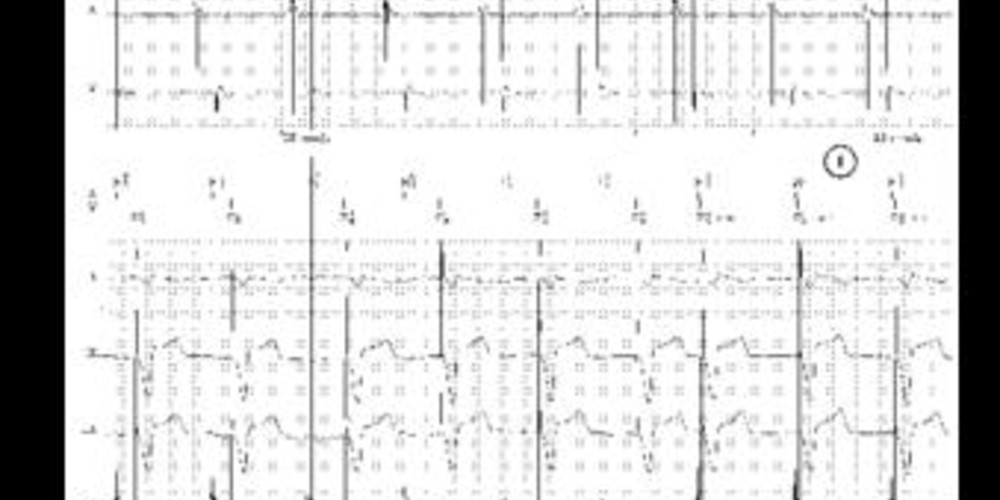
Tracing 20a
- first phase of the signal quality check with capture assessment; for 5 consecutive cycles, a single ventricular pulse is delivered (an emergency pacing is delivered only in the absence of capture); the AV delay is shortened (15 ms for spontaneous atrial activity as in this patient or 50 ms for paced atrial activity) to ensure complete ventricular capture; the starting amplitude of this test is programmable; the first of these cycles is ignored to allow stabilization of the signal at the new pacing amplitude; the evoked control response of the capture is assessed over the next 4 cycles;
- second phase of the signal quality check; for 5 consecutive cycles, 2 consecutive ventricular pulses with a 100 ms delay are delivered; the first allows an effective capture, the second is delivered in the absolute refractory period to assess the polarization artifact in the absence of capture; these two successive phases allow differentiating between capture and non-capture, an imperative prerequisite for carrying out an automatic threshold measurement; if a single non-capture is found during the first phase or if the polarization signal is too strong, the validation step of signal quality is not verified and the automatic threshold measurement cannot be performed;
- once the quality of the signal is verified, the threshold measurement begins with a successive decrease in pacing amplitude in decremental 0.6 V steps as long as no loss of capture is diagnosed; the AV delay remains short to ensure complete capture;
- if no loss of capture is diagnosed at 0.6 V, the pacing amplitude is decreased with a 0.1 V step;
- the tracing shows a loss of capture on the first pulse at 0.5 V; a second pacing is delivered 100 ms after the first pulse at an amplitude of 0.6 V (0.1 V above the tested amplitude with a pulse duration of 1 ms); in this patient, both pulses at 0.5 V are ineffective, the threshold is therefore determined at 0.6 V and the threshold measurement stops.
Patient: 74-year-old woman implanted with an Evia DR-T dual-chamber pacemaker for complete atrioventricular block; during the consultation, automatic right ventricular threshold measurement.
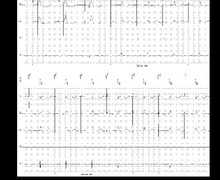
Tracing 20b
- first phase of the signal quality check with capture assessment; for 5 consecutive cycles, a single ventricular pulse is delivered (the first of which is not visualized on this tracing); the AV delay is shortened to 50 ms since atrial activity is paced; the starting amplitude of this test is programmed to 3 V (nominal value);
- second phase of the signal quality check (5 cycles with double ventricular pacing);
- once the quality of the signal is verified, the threshold measurement begins with a successive decrease in pacing amplitude in decremental 0.6 V steps as long as no loss of capture is diagnosed;
- loss of capture diagnosed at 0.6 V over 2 consecutive cycles;
- the pacing amplitude thus returns to the last value allowing a capture (1.2 V in this instance);
- the pacing amplitude is decreased with a 0.1 V step;
- in this patient, both pulses at 0.9 V are ineffective, the threshold is therefore determined at 1 V and the threshold measurement stops.
Other articles that may be of interest to you
EGM recordings

In all modern pacemakers, it is now possible to program an automatic ventricular threshold measurement function more or less associated with an automatic adjustment of the pacing amplitude.
When the ventricular capture control is programmed to OFF, the thresholds are not automatically measured by the device. When the ventricular capture control is programmed to ON, automatic measurement of the ventricular pacing threshold is followed by an adjustment of the pacing amplitude with cycle-to-cycle control of capture efficiency. The principle of the threshold measurement is to determine the minimum amplitude allowing an effective capture with an accuracy of 0.1 V. When the ventricular capture control is programmed to ATM, the device automatically measures the threshold value but without any possible adjustment of the pacing amplitude which remains fixed regardless of the measured value.
The scheduling of the automatic measurement and the frequency of the measurements are programmable.
When the ventricular capture control is programmed to ON, there is therefore a cycle-to-cycle verification of the capture based on the analysis of the evoked response. A safety margin with respect to the threshold measurement is programmable (nominal value 0.5 V). This programming option is only possible if the pulse duration is programmed to 0.4 ms or less; indeed, if a loss of capture is found, a safety pulse is delivered by increasing the pulse duration; hence, a sufficient margin is required.
Another key element to be aware of is that the maximum amplitude that can be delivered is 4.8 V for 0.4 ms, thus well below the maximum capacities. This programming option must therefore be avoided when the pacing threshold is very high.
Various parameters are thus programmable: