Induction of ventricular fibrillation by shock on the T wave
Tracing
Manufacturer Abbott
Device ICD
Field Implantation
N° 3
Patient
A 74-year-old man in New York Heart Association functional class III, who suffered from ischemic cardiomyopathy, LVEF at 19% and left bundle branch block, underwent induction of VF at the end of ICD implantation.
Main device programming (during the induction procedure)
- Single VF zone for rates >187 bpm
- 12 cycles in the VF zone were needed for the diagnosis
- Sensitivity programmed at 0.5 mV
- First shock at 36 J, second shock at 40 J (maximum strength).

Graph and trace
Narrative
The narrative indicates the occurrence of VF lasting 18 sec, with delivery of a probably successful 36-J shock; the >995 ms post-shock coupling was measured from the 4 cycles that preceded the diagnostic of return to sinus rhythm. The charge time was 7.5 sec and the shock impedance 43 Ohms.
Trace
1: Atrial and biventricular paced rhythm;
2: Short charge of the capacitors to deliver a low-energy shock to induce VF (*);
3: Burst of 8 stimuli at 100 bpm;
4: A 2-J shock was delivered on the peak of the T wave at a 310-ms coupling cycle length;
5: A 1-sec post-shock blanking precluded any sensing;
6: VF episode; at the third F, switch to DDI episode pacing mode;
7: Presence of very short and often low-voltage cycles; noteworthy alternans between a first sensed signal and a second signal, which is not sensed, despite being of high amplitude, because it is in the ventricular blanking period, visible on the markers chain;
8: The following cycle is unclassified after this undersensing, because it is outside the VF zone, whereas the average of the 3 previous and the on-going cycles remained in the VF zone;
9: Detection of the episode after 12 cycles in the VF zone. The detection is slightly delayed because of sensing failures; trigger of the EGM recording and onset of the capacitors charge;
10: Confirmation of the persistence of the arrhythmia during the charge (underscored F);
11: Higher-amplitude ventricular EGM, the next is undersensed;
12: End of the capacitors charge;
13: The shock cannot be delivered on the first cycle following the end of the charge;
14: Delivery of 36-J shock;
9: Successful shock and termination of the arrhythmia.
Other articles that may be of interest to you


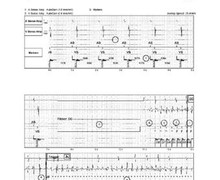

In this patient, who suffered from heart failure and conduction disorders, induced VF was highly polymorphic, with markedly fragmented ventricular EGM of variable amplitude, such that the visual distinction of R from T waves was nearly impossible. This kind of arrhythmia is difficult to diagnose for a defibrillator. This test was performed at the highest ventricular sensitivity of 0.5 mV, leaving a narrow programming margin and, consequently, limited sensing capability, as the value that is usually programmed on the long term is 0.3 mV. When VF is poorly sensed and the diagnosis is compromised or delayed, the lead position must be changed.
The R wave is not measured by analysing the signals’ peak to peak; instead, it represents the highest positive or negative peak.