T-wave oversensing with decrease in the percentage of biventricular stimulation
Tracing
Manufacturer Abbott
Device CRT
Field Standard parameters
N° 5
Patient
Patient 1 :
This 71-year-old man received a Abbott Unify Assura triple chamber CRT-D in the context of a dilated cardiomyopathy with wide QRS complex. A decrease in the percentage of BiV stimulation and episodes of ventricular oversensing stored in the device’s memory were observed during a routine ambulatory visit.
Patient 2 :
This 76-year-old man received a Abbott Unify Assura triple chamber CRT-D in the context of ischemic cardiomyopathy with left bundle branch block. A decrease in the percentage of BiV stimulation and recordings of episodes of ventricular oversensing were found in the device memory at the time of a routine ambulatory visit.
Graph and trace
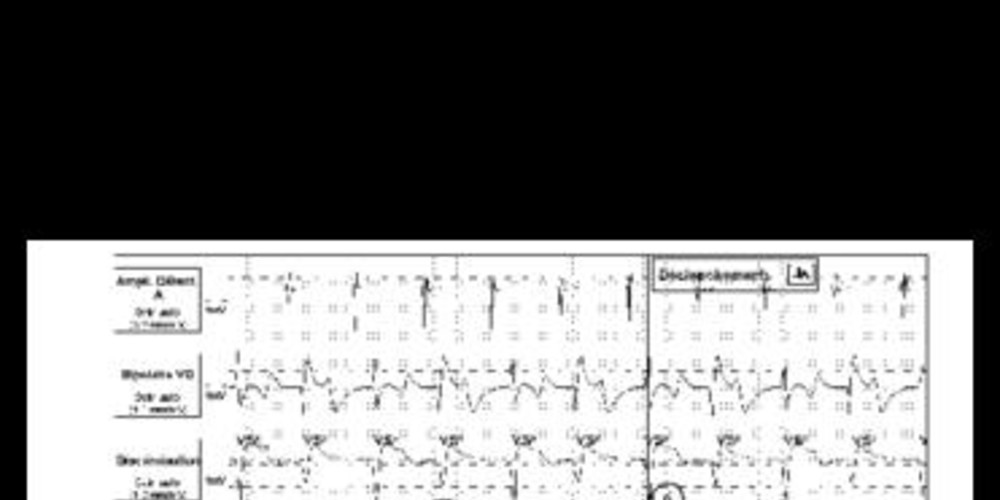
Tracé 5a :
- BiV stimulation.
- oversensing of the T wave (- marker, unclassified cycle because of a discordance between the current cycle and the average of the 4 previous cycles) after ventricular pacing.
- spontaneous atrial event sensed in the PVARP. The previous ventricular event (T wave) was diagnosed as a PVC with lengthening of the PVARP.
- AV conduction with spontaneous QRS; cycle also unclassified.
- same sequence with alternans between paced and sensed ventricular cycle.
- the SecureSense algorithm diagnoses non-sustained ventricular oversensing.
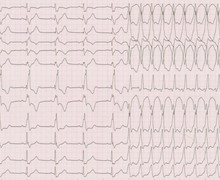
Tracé 5b
- BiV stimulation with atrial pacing at the sensor rate.
- BiV stimulation with atrial pacing.
- oversensing of the T wave of a paced ventricular event (- marker, unclassified cycle because of discordance between the current cycle and the average of the 4 previous cycles).
- spontaneous atrial event sensed in the PVARP; the previous sensed ventricular event (T wave) is diagnosed as PVC with lengthening of the PVARP.
- AV conduction with spontaneous QRS complex.
- same sequence with alternans between a paced and a sensed ventricular cycle.
- the SecureSense algorithm diagnoses non-sustained ventricular oversensing.
Other articles that may be of interest to you

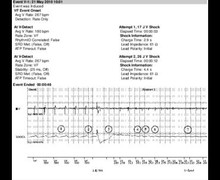

The programming of the new SecureSense discrimination algorithm on this series of defibrillator models inhibits therapies and prevents the delivery of inappropriate therapies triggered by oversensing of myopotentials, lead fracture potentials, or of the P, T, or R-waves. The algorithm, however, does not interfere with pacing. In these 2 patients, oversensing of the T-wave was the cause of a prominent decrease in the percentage of BiV stimulation with alternans between a paced and a sensed ventricular event. An attempt could be made to change the post-pacing adaptation delay to prevent oversensing.