Ventricular sensing failure
Tracing
Manufacturer Medtronic
Device PM
Field Pacing & Sensing
N° 14
Patient
81-year-old woman, implanted with an Adapta dual-chamber pacemaker for atrial disease; evolution towards well-controlled chronic AF; programming in VVIR mode 60-120 beats/minute; asymptomatic, routine visit.

Graph and trace
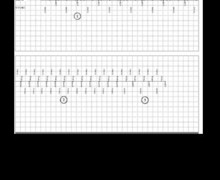
The first line corresponds to lead III with the superimposed markers, the second line to the ventricular EGM and the last line to lead II with the superimposed intervals;
- ventricle undetected despite correct amplitude on ventricular EGM; ventricular pacing in vulnerable period of the previous QRS with effective ventricular capture;
- rate responsive ventricular pacing;
- reappearance of undetected spontaneous ventricles with pacing at regular intervals;
- new pacing in vulnerable period without capture.
Other articles that may be of interest to you



The sensitivity expressed in millivolts (mV) depicts the ability of the pacemaker to properly detect spontaneous cardiac events. Appropriate programming of the sensitivity level should allow detecting all spontaneous cardiac events occurring in the implanted chamber while not detecting events of a different nature (crosstalk with sensing of cardiac signals from the other chamber, myopotentials, interference, etc.). The programming of bipolar sensing allows enhancing the specificity of detection relative to unipolar sensing by limiting the risk of sensing extra-cardiac or crosstalk signals while allowing the programming of high sensitivity values. On the other hand, in the unipolar configuration, the risk of crosstalk or extracardiac signal sensing requires the programming of a lower sensitivity level with an increased risk of undersensing.
This tracing reveals an example of ventricular undersensing in conjunction with inappropriate programming. Indeed, the ventricular signal was measured at 3.8 mV in bipolar mode while the ventricular sensitivity was programmed at 5 mV. In the absence of proper sensing, the pacemaker operates in VOO mode with impossibility of inhibition due to the spontaneous ventricles. This leads to unnecessary energy consumption and is associated with an increased pro-arrhythmia risk if pacing occurs in a vulnerable ventricular period. This tracing raises the issue of the optimization of the programming of ventricular sensitivity.
Traditionally, unlike implantable defibrillators, pacemakers functioned with a stable and fixed sensitivity over the entire cardiac cycle. Nowadays, the various manufacturers propose, in their range of devices, a fusion between the operational platforms of pacemakers and defibrillators. Even though the sensing constraints are not the same (crucial necessity for a defibrillator to detect and treat very rapid, polymorphic and low-voltage ventricular rhythm disorders), modern pacemakers allow an adaptive sensitivity (variable sensitivity level according to R-wave amplitude or the sensed P wave) with a progressive increase in sensitivity during the cardiac cycle (possibility of detecting small amplitude signals without T-wave oversensing). Depending on the age range of the MedtronicTM pacemaker, the functioning of the ventricular sensitivity differs. Proper knowledge of this element is essential at the time of programming. It is indeed imperative to know the type of programmed sensing, the maximum sensitivity value to be programmed differing completely.
For the more recent devices, ventricular sensing is necessarily adaptive (non-programmable) if bipolar sensing is programmed and necessarily fixed if unipolar sensing is programmed. On a pacemaker, a nominal value of 0.9 mV is programmed, the device being less sensitive than a defibrillator (nominal value 0.3 mV) in order to avoid the risk of inappropriate inhibition in a pacemaker-dependent patient.