Dual-chamber VDD mode
Tracing
Manufacturer Medtronic
Device PM
Field Pacing Modes
N° 6
Patient
Same patient as in tracing 1.
Graph and trace
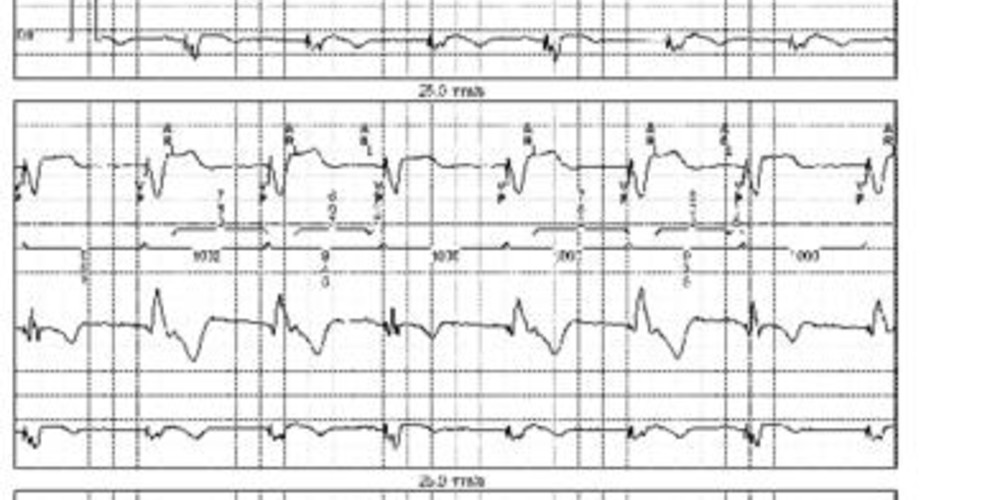
Tracing 6a: programming in VDD mode 60 beats/minute;
- atrial sensing and ventricular pacing (AS-VP);
- slowing of atrial activity and ventricular pacing at the base rate (1000 ms between 2 VPs) without atrial pacing; atrial retrograde conduction detected in the post-ventricular atrial refractory period (AR) not triggering an AV delay or ventricular pacing;
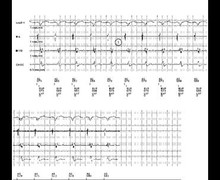
Tracing 6b: programming in VDD mode 40 beats/minute;
- proper sensing of atrial depolarization and ventricular pacing (AS-VP); the slowing of the base rate avoids any non-synchronized ventricular pacing on atrial sensing;
- proper sensing of the atrial extrasystole and ventricular pacing.
Other articles that may be of interest to you


The VDD mode can be programmed on a conventional dual-chamber pacemaker but can also be obtained from a single-chamber device or a ventricular single-lead VDD pacemaker with two floating atrial electrodes for atrial sensing and the ventricular bipolar pacing/sensing electrodes. On the other hand, any atrial pacing is impossible. Sensing is therefore carried out in the atrium and in the ventricle, although pacing only takes place in the ventricle. The VDD mode provides synchronized pacing in the atrium (or VVI pacing at the minimum rate). The ventricle is paced synchronously up to the maximum synchronous rate.
This mode is therefore acceptable in the absence of sinus dysfunction; it is advisable to program a low base rate, possibly with rate hysteresis to avoid VVI behavior. Indeed, on this tracing, the programming at 60 beats/minute is associated with retrograde conduction and pacemaker syndrome. In this example, retrograde conduction is detected in the PVARP and therefore does not induce PMT. A PMT protection algorithm must be programmed.
The advantages of single-lead VDD systems are that:
The disadvantages of single-lead VDD systems are that:
The preferred indication of the VDD mode is therefore complete AV block with normal sinus function.