VT counter
Tracing
Manufacturer Medtronic
Device ICD
Field Counter
N° 8
Patient
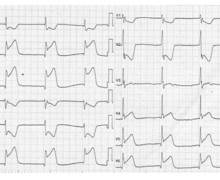
Patient implanted with a dual-chamber ICD (Evera XT DR) for right ventricular arrhythmogenic dysplasia with multiple episodes of ventricular tachycardia; 3 detection zones were programmed with a VT zone between 360 and 300 ms; the analyzed episode was diagnosed as VT by the device; the purpose of this tracing is to highlight the need to properly program the lower limit of the VT zone.
Graph and trace
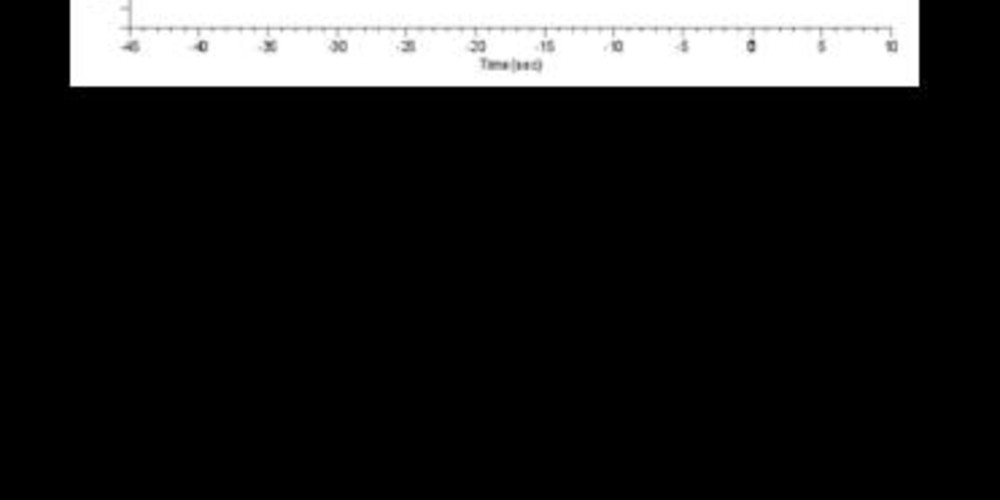
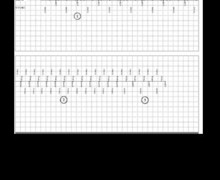
The graph initially shows a regular 1:1 atrioventricular rhythm (sinus rhythm) followed by a sudden acceleration of the ventricular rate with atrioventricular dissociation. Some ventricular intervals are detected in the VT zone, others are outside (VS intervals) explaining why the number of required intervals before detection appears relatively large. An anti-tachycardia pacing burst allows a return to sinus rhythm.
- on the EGM, there is an initial sinus rhythm;
- sudden acceleration with atrioventricular dissociation;
- irregular ventricular intervals can be observed alternately classified as TS or VS;
- the VT counter is reset to 0 in an iterative manner following the occurrence of intervals classified as VS;
- the ventricular rhythm accelerates and stabilizes in the VT zone;
- the VT counter is filled after 16 consecutive TS intervals;
- burst is delivered, with a return to sinus rhythm;
- end-of-episode diagnosis after 8 consecutive intervals classified as VS or VP.
Other articles that may be of interest to you


This tracing shows one of the limitations of the VT counter which requires a programmable number of consecutive intervals classified as TS and allows emphasizing the importance of the programming of the lower limit of the VT zone. Indeed, in this patient, the diagnosis of VT is indisputable with an obvious atrioventricular dissociation. There is, however, a diagnostic delay generated by the functional specificity of this counter. The tachycardia is irregular and oscillates with the lower limit of the VT zone. When an interval is classified as VS, the VT counter is reset to 0 even though the diagnosis is obvious, as in the present case. It is therefore essential to program a sufficient margin with regard to the rate of clinical tachycardia in order to avoid this type of problem. It is common to program the VT zone 10 to 20 beats per minute slower than the clinical VT, this margin probably needing to be slightly increased for MedtronicTM devices, the occurrence of a cycle classified as VS not having the same consequences compared to other competing devices. This specificity also implies that the VT counter not be used for tachycardias greater than 200 beats per minute, the risk of intermittent undersensing being increased (polymorphic tachycardias more frequent) and resulting in a delay or absence of diagnosis and therefore of treatment. The probabilistic VF counter appears to be more appropriate for this type of tachycardia.
In the latest international guidelines, there are marked differences in terms of advice for setting the limits of the detection zones according to device manufacturers. The different functioning of the counters explains some of these differences (in primary prevention, MedtronicTM has a single VF zone at 188-200 beats/minute, Boston ScientificTM a VT zone up to 230 beats/followed by a VF zone).