lead fracture and aystole
Tracing
Manufacturer Medtronic
Device ICD
Field Oversensing
N° 27
Patient
Patient implanted with a triple-chamber ICD (Viva XT CRT-D) for primary dilated cardiomyopathy and hospitalized for syncope; this tracing illustrates the risk of asystole in conjunction with an oversensing caused by lead dysfunction.
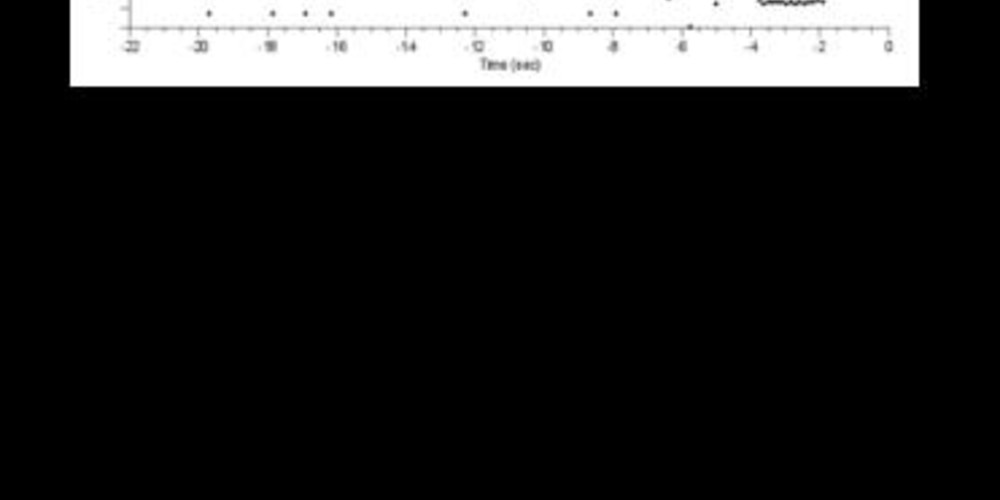
Graph and trace
The graph shows initially a large variability of the ventricular intervals with very short intervals followed by longer intervals; stabilization of a very fast ventricular rhythm explaining the sensing of an unsupported episode of VT.
- the EGM initially reveals the oversensing of isolated short ventricular intervals related to low amplitude potentials; a right ventricular pacing occurs when a signal is oversensed during the post-atrial pacing window explaining the very short intervals;
- the oversensing persists for 2 to 3 seconds explaining the occurrence of a ventricular pause.
Other articles that may be of interest to you




This patient presented an oversensing of pectoral myopotentials which could be reproduced by counter maneuvers of the arm ipsilateral to the pulse generator. In this patient with altered atrioventricular conduction, oversensing induced ventricular pauses of variable duration, responsible for repeated lipothymias/syncopes. Two types of myopotentials can be oversensed by an ICD:
Analysis of the EGMs in this setting reveals the presence of very fast (high-frequency) non-physiological signals. Oversensing can be replicated by isometric movements of the arm ipsilateral to the can or by manipulation of the lead in the pocket. When there is suspicion of pectoral myopotential oversensing, a chest X-ray should be performed along with a thorough verification of the device (impedance values, pacing and sensing thresholds). The presence of an abnormally low impedance value (pacing and/or defibrillation) or a sudden decrease in this value is suggestive of an insulation defect. In very rare cases, oversensing of myopotentials can be observed when a DF1 system has been implanted with inversion of the pins in the connector.