Electrical shock for VF
Tracing
Manufacturer Boston Scientific
Device ICD
Field Therapy
N° 1
Patient
This 64-year-old man with severe ischemic cardiomyopathy underwent implantation of a Boston Science Teligen dual chamber defibrillator for secondary prevention after episodes of polymorphous VT. A few months after implantation, he was seen after having lost consciousness and received an electrical shock.
Summary
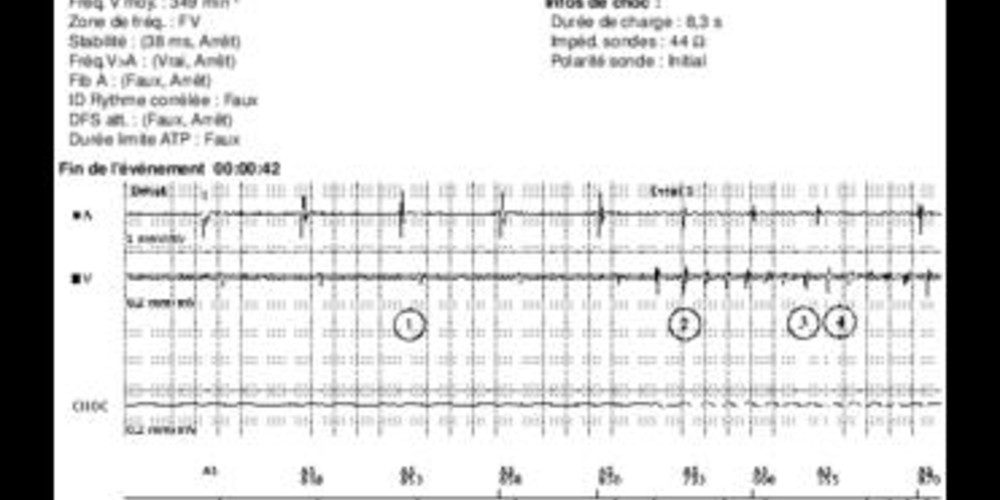
This episode was classified in the VF zone, prompting a 41-J shock after a >8 sec charge time. The delay between the onset of arrhythmia and the electrical shock was, therefore, 10 sec, which might explain the loss of consciousness.
Graph and trace
Tracing
- sinus rhythm (AS-VS);
- very rapid, spontaneous, polymorphous, ventricular tachyarrhythmia; the first cycle was in the VT zone and the following cycles in the VF zone;
- detection of an episode (V-Epsd; 8 out of 10 criterion fulfilled); the criterion was fulfilled for the VT zone (1 cycle in the VT zone + 7 cycles in the VF zone); the duration of initial detection for the VT zone began with this cycle; switch to the VDI mode;
- with this cycle, the initial detection window was fulfilled for the VF zone (8 cycles in the VF zone); the Duration of initial detection began with this cycle. The Duration of the VF zone trumped the Duration of the VT zone. Even if the Duration of the VT zone ended before that of the VF zone, if the 6 out of 10 criterion is fulfilled for the VF zone, the VT zone therapies are withheld until the Duration of the VF zone ends;
- persistence of arrhythmia detected in the VF zone during the Duration, which was of 1 sec in the VF zone (V-Detect);
- onset of the charge of the capacitors;
- ventricular sensing remained reliable during the charge, except for a few undersensed cycles explaining the VS or VT markers. These sensing failures were too sporadic to cause a diversion of the charge;
- end of the charge lasting >8 sec. The strength of the shock delivered corresponded to the maximum capability of the device;
- at the end of the charge, a 135-ms refractory period began. The first cycle following that refractory period was not counted (--); the next 2 cycles were short (VF), and the charge diversion window ended, 500 ms after the end of the charge. The 2 out of 3 criterion was fulfilled;
- 41-J electrical shock delivered on the second cycle (synchronized to the R wave);
- the first ventricular and first atrial cycles following the post-shock refractory period (500 ms) are not counted (--);
- 2 sec post-shock phase during which pacing is precluded, followed by DDD pacing;
- successful electrical shock and termination of the arrhythmia;
- lengthening of the PVARP after a cycle classified as VES;
- in this patient whose PR interval was prolonged, the P wave was sensed in the PVARP, explaining the inscription of “AS” in parentheses (AS).
Other articles that may be of interest to you


This tracing illustrates the normal function of a defibrillator during an episode of VF: the arrhythmia was accurately detected, followed by charge of the capacitors, confirmation of the arrhythmia at the end of the charge and delivery of a successful shock. A series of up to 8 shocks can be programmed in the VF zone. The strength of the 3rd to 8th shocks is not programmable and is necessarily the highest (41 J). On the other hand, the strength of the first 2 shocks is programmable, though the amplitude of the second must be ≥ than the first.
Because the delay between the onset of arrhythmia and the shock delivery lasted >10 sec, this patient lost consciousness. This delay includes a) the initial detection time (non-programmable 8 out of 10 criterion), b) the Duration (while it is programmable, it lasted 1 sec in this case, therefore without programming margin), c) the charge time of the capacitors (which depends on the programmable strength of the first shock), and d) the non-programmable confirmation at the end of the charge, which lasts ≥500 ms). The only means of shortening this delay is, therefore, to change the strength of the first shock. By lowering the strength of this first shock (after verification of its efficacy during a VF induction test) the charge time can be shortened and the shock hopefully delivered before loss of consciousness, knowing that the likelihood of success of that first therapy is lower. The patient’s age, personal and professional activities, and automobile driving habits might have an influence on that decision. In this patient, the strength of the first shock was left unchanged, with a view to give priority to safety, and accepting the risk of another syncopal event in case of recurrent arrhythmia of this type.